
Introduction by William Martin
In the early 1970s, a National Commission on Marihuana and Drug Abuse, appointed by President Richard Nixon, urged federal and other levels of government to “maintain and monitor an ongoing collection of data necessary for present and prospective policy planning, including data on incidence, nature, and consequences of drug use.” That recommendation has been well satisfied. The National Survey on Drug Use and Health (NSDUH),1 launched in 1971, conducts face-to-face interviews with approximately 70,000 people 12 years and older annually. Monitoring the Future (MTF), begun in 1975, questions approximately 50,000 teens annually, with follow-ups in later years. These surveys, which easily qualify as Big Data, provide a rich and revealing picture of drug use in America, and their findings are consistently confirmed by other surveys. Still, although the information is available to anyone with a computer, few people appear to know the size or actual contours of drug use in this country, and the data play only a small role in public policy, mass media presentations, and popular perception.
Until one becomes familiar with the format of the NSDUH, MTF, and other valuable collections of statistics relevant to drug policy, quickly absorbing their implications can be daunting. Even after one gets the hang of it, the longitudinal graphs often cover only a modest number of years, making it difficult to trace trends across the four-plus decades of the War on Drugs.
About a decade ago, a friend introduced me to a website constructed by Brian C. Bennett, a former career intelligence analyst now at the University of Virginia, who has compiled and painstakingly sorted through a vast amount of official government data produced since 1970 regarding substance use and abuse. Bennett then displayed these data in easily understood graphs, charts, and tables that collectively force one to recognize that many widely accepted beliefs and stereotypes about drug use in the United States are simply not true. The most common of the charts show the percentage of people, either 12 and older or broken into smaller age groupings, who have ever used a given drug at some time in their lives, in the past year, and in the last month.
High proportions of people who have ever used any of the drugs against which federal, state, and local law enforcement agencies have waged war for more than 40 years stopped using within the first year and no longer use regularly, if at all. When I have shown these charts to students, members of service clubs where I have spoken, or colleagues and supporters of the Baker Institute, the reaction is invariably surprise, sometimes approaching amazement. On occasion, some have told me that those charts did more than anything else to cause them to look at drug use and abuse and the War on Drugs in a quite different light.
To my disappointment, career demands caused Bennett to stop updating the charts after the 2008 surveys. Fortunately, when I contacted him he said he would be pleased to have the Baker Institute Drug Policy Program share and update the work he had done and give it a home where the work could continue. In the ensuing period, Katharine A. Neill, the Alfred C. Glassell, III, Postdoctoral Fellow in Drug Policy, and an intern, Madeleine Tibaldi, updated a sizable number of the charts with data from the latest surveys, and the institute’s graphic designers devised a new format for the charts, which Bennett approved. We are happy to present these in a new section of our website, appropriately named The Brian C. Bennett Drug Charts, and also to welcome Brian Bennett as a new nonresident contributing expert to our program.
At present, the charts and graphs on our website are a small but growing fraction of those available on briancbennett.com, which recently received its four millionth visit. We invite you to explore that site for more charts and many other fascinating features, with the warning that you may find it addictive. We expect to transfer more updated materials to our website in the near future, but always with the explicit recognition of and appreciation for the enormous effort Bennett put into creating and maintaining the original site for many years.
Can We Trust These Data?
Any survey asking people to provide information about behavior that could possibly subject them to legal sanctions, social disapproval, or personal embarrassment or guilt has to answer at least three questions: 1) Who is being interviewed? 2) Who is not being interviewed? and 3) Are the people being interviewed telling the truth? These are legitimate questions and we address them in some detail on our website. For our purposes here, we limit ourselves to saying that whatever their flaws, NSDUH and MTF are the best surveys we have and the best we are likely to get. The consistency of their findings over decades offers considerable assurance that they provide a dependably accurate picture of drug use in America. They are the data of record for all levels of government and law enforcement agencies, and the numbers that must be used to formulate rational public policy. As noted above, for far too long they have played too small a role in public policy, mass media presentations, and popular perception. We hope, by widening exposure to these data, to alter that situation.
Marijuana
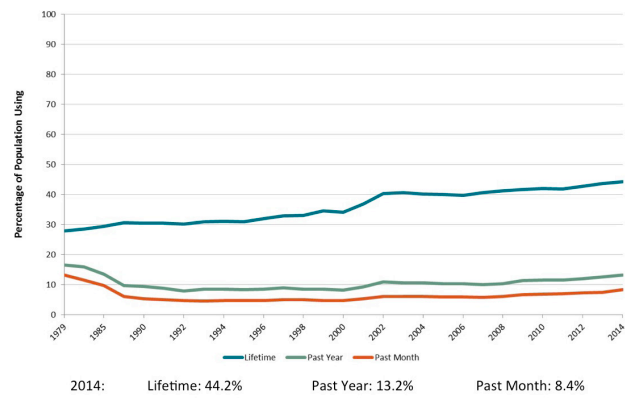
By far the most widely used drug still illegal in most states, marijuana—more properly, cannabis—follows the expected pattern of low rates of regular use (Figure 1). Slightly more than 44 percent of respondents 12 or older and more than half of those under 60 acknowledge having used marijuana at least once in their lives.2 As expected, less than a third of those had used it in the past year and less than a fifth had used in the month prior to participating in the survey. Far from being a “gateway” to the use of harder drugs such as cocaine and heroin, marijuana is for most people who try it not even a gateway to more marijuana use.3 It is still too early to tell how increased decriminalization and legalization of cannabis in a growing number of states will affect usage rates. Thus far, rates in Colorado and Washington, the first states to legalize marijuana, are edging upward, but not nearly as dramatically as critics had predicted.4 Colorado Governor John Hickenlooper, who had opposed legalization in the state, acknowledged after a year of full commercialization that “It seems like the people that were smoking before are mainly the people that are smoking now.”5 It would be surprising if usage rates did not rise somewhat, accompanied by an increase in the problems associated with heavy cannabis use, but unless and until that happens, it is likely that the pattern of predictable decline, established over decades, will prove to be enduring.
Figure 1 — Marijuana Use Among Persons Aged 12 Years and Older (1979–2014)
Cocaine
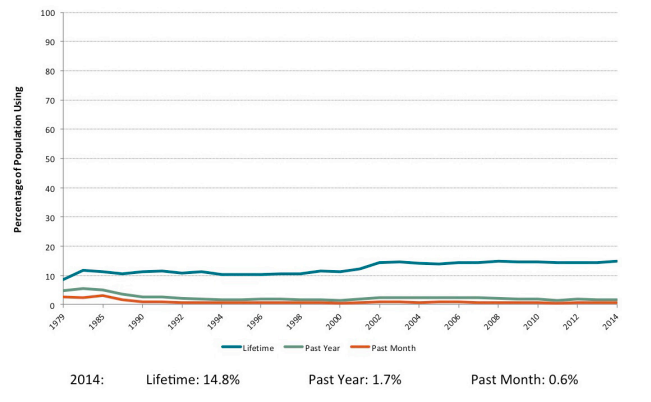
Cocaine, the “White Queen” of the Colombian/Mexican drug trade for many years, appears to have lost some of her allure (Figure 2). According to a study conducted by the RAND Corporation for the White House Office of National Drug Control Policy, the total amount of pure cocaine consumed in the United States fell by roughly 50 percent between 2000 and 2010, with an attendant drop in cocaine expenditures from $55.1 billion to $28.3 billion over that decade.6 Without minimizing for a moment the havoc cocaine addiction can wreak on the lives of individuals and their social circles, even a cursory look at this chart indicates that, absent the crime and corruption related to evading enforcement of prohibition, the threat it poses to society has been overstated. Less than 15 percent of U.S. residents 12 or older have ever used cocaine, including crack, which is simply cocaine in a smokable form. After a decade of relative popularity in the 1980s, the percentage of new or occasional users, signified by past-year users, dropped from 5.86 percent in 19797 to less than a third of that by the mid1990s,8 rose slightly in the first decade of the current century, then settled back down to less than 2 percent. Even more striking, despite media-stoked fears of a nation about to be ravaged by cocaine addiction, the number of people who can reasonably be thought to have a dependence on cocaine or crack has long remained close to its 2014 level of 0.6 percent—six out of every 1,000 people over the age of 11. Even more significant, since new people self-identify as regular (monthly) users each year, yet the overall number of people in the frequent-user category remains stable, it is clear that not all use is abuse and that most people who get into trouble with the drug recover from it, many on their own without treatment, participation in a 12-step recovery program, or relapse.9
Figure 2 — Cocaine Use Among Persons Aged 12 Years and Older (1979–2014)
Methamphetamine
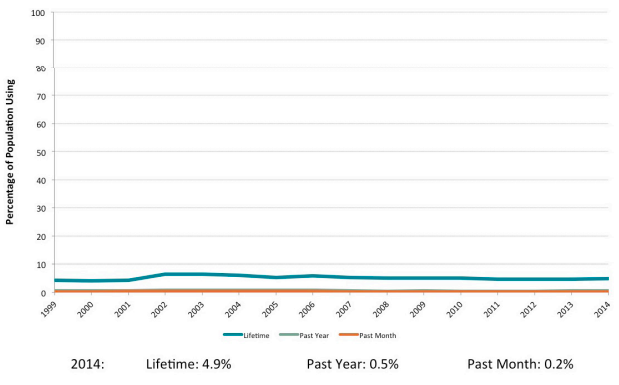
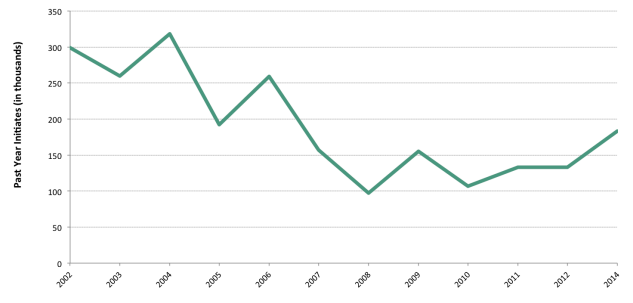
The NSDUH began tracking methamphetamine use in 1999 in response to concerns about the growing rates of use in the 1990s. Since that time, the pattern of meth use by individuals has remained relatively stable (Figure 3). In 2014, 4.9 percent of those surveyed reported having used meth at some point in their lifetime, and only 0.2 percent reported having used meth in the past month. Its popularity, however, tends to vary periodically, as shown in Figure 4. In 2004, for example, the number of new users hit a high of over 318,000, dropped to 192,000 in 2005, rose sharply to 259,000 in 2006, then nosedived to only 92,000 in 2008 and remained at levels less than half its 2004 peak for seven years, suggesting an overall trend toward a decline in meth use. The number of first-time meth users spiked in 2014, creeping up to 183,000—still less than 0.1 percent of people aged 12 years and older.
Figure 3 — Methamphetamine Use Among Persons Aged 12 Years and Older (1999–2014)
Meth use also varies across states and is most prevalent in whiter, more rural areas. In Oregon, for example, meth was listed as the number-one drug concern among 62 percent of law enforcement agencies surveyed by the Oregon High Intensity Drug Trafficking Area Program in 2015.10 Another proxy measure of the meth problem in an area—the number of meth-related seizures or laboratory incidents—suggests that meth use is more popular in the Midwest and Southern states.11 The relative ease and cheapness of cooking meth makes it an attractive drug of choice in poor rural areas, but the vast majority of Americans have never tried it, let alone used it problematically.
Figure 4 — Past Year Methamphetamine Initiates Among Persons Aged 12 Years and Older (2002–2014)
Prescription Opioids and Heroin
In 2014, 20.5 percent of the U.S. population age 12 or older, or roughly 56 million people, reported using prescription pain relievers, tranquilizers, stimulants, or sedatives for a nonmedical purpose at some point in their lives. But only 2.5 percent, 6.8 million, said they had done so in the past month, a rate little changed since 1985.12 Despite the legal status of these drugs and the benefits attributed to them in TV commercials (before the oral equivalent of fine print warns of their many dangers), finding fun in the medicine cabinet is risky business.
According to the Centers for Disease Control and Prevention (CDC), 47,055 drug overdose deaths occurred in the United States in 2014, a rate of 14.7 per 100,000 persons. At least a third of these, and almost certainly many more, involved the dangerous practice of mixing drugs such as painkillers and alcohol, or heroin and benzodiazepines or cocaine, or hydrocodone and acetaminophen (Tylenol), combinations that can have a powerful synergistic and fatal effect.13 The rate of overdose deaths officially attributed to opioids alone was 9.0 per 100,000 persons in 2014.14
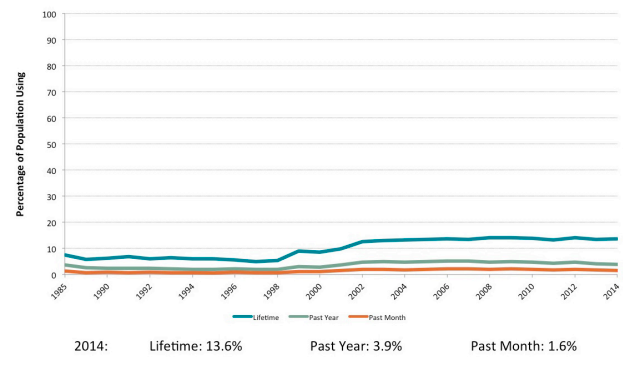
Figure 5 isolates nonmedical use of prescription painkillers from that of other prescription drugs. The percentage of people who reported having ever used prescription painkillers for nonmedical purposes was higher in 2014 than it was in 1985, the first year for which data were available, but the increase has been moderate for lifetime use and small for past-year and past-month use. In 2014, 37.2 million people, or 13.6 percent of the U.S. population aged 12 years and older, reported having used prescription painkillers for nonmedical reasons during their lifetime. The number of individuals who reported nonmedical use of painkillers in the past month, however, was 4.4 million. This is not a small number of potentially problematic users, but it is a small segment of the U.S. population—1.6 percent of those aged 12 years and older. It is important to maintain perspective regarding the scale of problematic use.
Figure 5 — Nonmedical Prescription Pain Reliever Use Among Persons Aged 12 Years and Older (1985–2014)
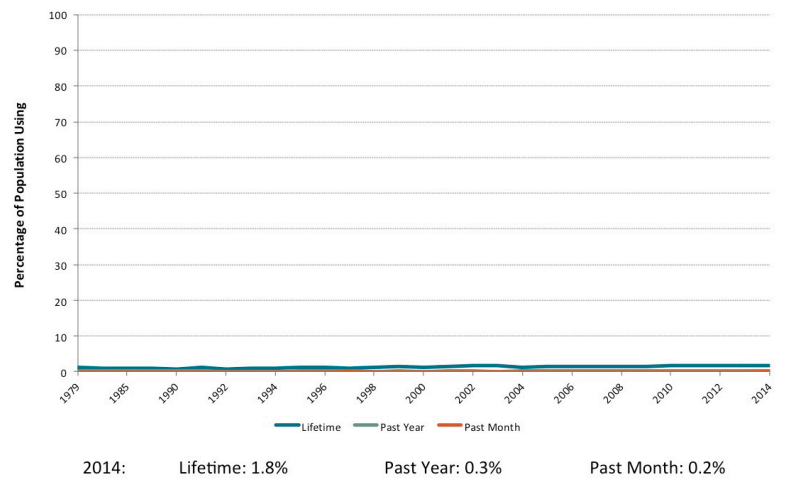
Maintaining perspective is also important when thinking about heroin. Dramatic media attention to increases in heroin use can skew public perceptions by failing to provide accurate and appropriate information about the scope and context of that use. As Figure 6 indicates, national trends in heroin use remained quite stable between 1979 and 2014. In 2014, 1.8 percent of U.S. residents 12 years and older (4.9 million people) acknowledged having used heroin at some point in their life. Only 0.2 percent (546,600 people) reported having used it in the past month. It is certainly possible, even likely, that this low figure reflects some underreporting. But even if we assume that this estimate is off by a magnitude of five, which is not likely, that would still mean that only 1 percent of U.S. residents age 12 and up reported using heroin in the past month at the time of the 2014 survey.
Figure 6 — Heroin Use Among Persons Aged 12 Years and Older (1979–2014)
Not shown by these macro-level data is a change in the demographic profile of problematic heroin users, who, according to the CDC, are more likely to be “men, persons aged 18–25 years, non-Hispanic whites, persons with annual household income of less than $20,000, Medicaid recipients, and the uninsured.”15 Whites are now at the greatest risk of overdose and drug dependence. In 2014, the overdose death rate among whites was 19 per 100,000, compared to 10.5 for blacks and 6.7 for Hispanics.16 This usage pattern is a recent phenomenon. In 2000, black Americans aged 45-64 had the highest death rate for drug poisoning involving heroin.17 But in the past decade, 90 percent of those who tried heroin for the first time were white, and the share of people who say they have used heroin in the past year is actually decreasing for non-whites.18
Geographically, the Northeast, Southwest, and Midwest areas near the Appalachian Mountains have higher levels of problematic opioid use than other parts of the country. Predictably, states with the highest rates of overdose deaths in 2014 reflect this geographical pattern: 35.5 per 100,000 in West Virginia, 27.3 in New Mexico, 26.2 in New Hampshire, 24.7 in Kentucky, and 24.6 in Ohio.19 It is not a coincidence that these areas also have high rates of poverty and few economic opportunities. While greater willingness by physicians to write prescriptions for aggressively marketed opioids has clearly played a role,20 research indicates that the majority of people prescribed opioids for pain do not become addicted. Those who do are significantly more likely to have had a traumatic childhood experience, to have a mental illness, and/or to be facing economic insecurity.21 These are far stronger predictors of opioid dependence than the availability of heroin coming across the Mexican border or the street price for OxyContin.
Heroin use remains a problem in minority communities, particularly those with few economic and social resources, but the shift toward a whiter and younger user population has important implications for public perceptions of the problem and for policy responses. To put it bluntly, White Lives Matter. Parents, treatment providers, politicians, and pundits are starting to avoid words like “junkie” and “dopehead” in favor of gentler terms such as “persons with substance use disorders” and are saying that such disorders should be treated as a disease or a public health problem rather than as a crime. No politician wants to argue that we should start locking up white people the way we have locked up brown and black people for a century.
Fortunately, beneficial change is occurring. Forty-two states have increased public access to naloxone, an opioid antagonist that reverses overdose, and 32 states have passed Good Samaritan laws preventing prosecution for drug possession for someone who calls 911 to report an overdose. Several states are also looking to expand treatment and prevention services, and the city of Ithaca, New York, has proposed opening an on-site injection facility where users can have access to clean needles and use heroin under medical supervision,22 as is practiced successfully in several European countries.
Observations
The Bennett charts graphically illustrate the natural course of the use of psychoactive drugs. Most people who ever use such drugs stop using them shortly after initiation or a period of (usually brief) experimentation. Though not shown in the charts presented here, other figures found in NSDUH reports23 illustrate that this pattern is closely correlated with age, with illicit drug use (and other risky behaviors) reaching a peak between 18 and 25, declining sharply by age 26, then gradually dropping over the rest of the life span. This calls into question policies that levy harsh penalties and apply indelible criminal records to people for what may be experimental or incidental use likely to stop on its own in the normal course of maturation. More rational and compassionate responses exist and deserve close attention. (For examples, see Baker Institute Policy Report Number 63, Rx for U.S. Drug Policy: A New Paradigm, Appendix A).24
These charts also caution against uncritically accepting alarming announcements of drug abuse epidemics by media, politicians, religious leaders, law enforcement agencies, drug treatment facilities, voluntary associations, or others with real or opportunistic reasons to sound the klaxon. Drug epidemics do occur occasionally, but their natural course is to diminish after reaching a point at which most of the people likely to be vulnerable and receptive have been infected, when the bad effects of a drug clearly outweigh the pleasures of using it, or when intervention is effective. And most of the time, the actual dimensions of the problem are far less catastrophic than we are told.
This is not to trivialize the quite real, damaging, and sometimes irreversible consequences of harmful behavior that affects millions of Americans each year, importantly including those in the families and social circles of drug abusers and entire neighborhoods wracked by addiction and turf wars between criminal gangs competing to sell impure drugs at prices wildly inflated by prohibition. But policies that can deal effectively with these complex problems must build on a foundation of accurate data, not fear and stereotypes. The data exist. It is time to pay attention to them.
Endnotes
1. Until 2002, the name of the survey was National Household Survey on Drug Abuse. The name change reflects the recognition that not all use is abuse as well as the much increased attention to mental health.
2. For a graph of marijuana use by age cohort, see http://tywkiwdbi.blogspot.com/2012/08/marijuana-use-graphed-by-age-cohort.html.
3. For more about the gateway effect, see http://bakerinstitute.org/research/marijuana-gateway-drug/.
4. For an example, see “Legalizing Marijuana Will Intensify Use…” Retrieved from http://www.parentherald.com/articles/37865/20160419/legalizing-marijuana-intensify-use-teens-increase-drug-related-crimes.htm.
5. Jacob Sullum, “How Is Marijuana Legalization Going? The Price of Pot Peace Looks Like a Bargain,” Forbes, July 10, 2014. Retrieved from: http://www.forbes.com/sites/jacobsullum/2014/07/10/how-is-marijuana-legalization-going-so-far-the-price-of-pot-peace-looks-like-a-bargain/#1419f4d1167c.
6. What America’s Users Spend on Illegal Drugs: 2009-2010,” RAND Corporation, February 2014, p. 34, retrieved from https://www.whitehouse.gov/sites/default/files/ondcp/policy-and-research/wausid_results_report.pdf.
7. National Household Survey on Drug Abuse, 1979 Codebook (Rockville, Maryland: Substance Abuse and Mental Health Services Administration), Table 4, p. I-16. Retrieved from: https://datafiles.samhsa.gov/study-dataset/national-household-survey-drug-abuse-1979-nhsda-1979-ds0001-nid13802.
8. National Household Survey on Drug Abuse, 1995 Codebook (Rockville, Maryland: Substance Abuse and Mental Health Services Administration), p. 79. Retrieved from: http://samhda.s3-us-gov-west-1.amazonaws.com/s3fs-public/field-uploads-protected/studies/NHSDA-1995/NHSDA1995-datasets/NHSDA-1995-DS0001/NHSDA-1995-DS0001-info/NHSDA-1995-DS0001-info-codebook.pdf.
9. “Substance dependence recovery rates: With and without treatment.” The Clean Slate Addiction Site, 2016. Retrieved from: http://www.thecleanslate.org/self-change/substance-dependence-recovery-rates-with-and-without-treatment/.
10. Rick Bell, “New drug report: Meth still Oregon’s No.1 problem, run mostly by Mexican drug traffickers,” The Oregonian, June 21, 2015. http://www.oregonlive.com/pacific-northwest-news/index.ssf/2015/06/new_drug_report_paints_a_ less-.html.
11. Katy Hall, “The methiest states in the US,” The Huffington Post, October 7, 2013 Retrieved from: http://www.huffingtonpost.com/2013/10/07/methstates_n_4057372.html; “Top 10 states with the most meth labs,” Real Clear Politics, April 8, 2014. Retrieved from: http://www.realclearpolitics.com/lists/meth_states/south_carolina.html.
12. A chart for nonmedical use of all prescription drugs can be found in The Brian C. Bennett Drug Charts collection.
13. Kenneth Anderson, “How the Media Is Fueling the So-Called Opioid Overdose Epidemic,” Rehabs.com, July 21, 2015. Retrieved from: http://www.rehabs.com/pro-talk-articles/how-the-media-is-fueling-the-so-called-opioid-overdose-epidemic/; Anderson, “Ultimate Harm Reduction Guide to Drug Mixing,” Rehabs.com, March 4 2015. Retrieved from: http://www.rehabs.com/pro-talk-articles/the-ultimate-harm-reduction-guide-to-drug-mixing/.
14. Rose A. Rudd, Noah Aleshire, Jon E. Zibbell, and Matthew Gladden, “Increases in drug and opioid overdose deaths—United states, 2000-2014.” Morbidity and Mortality Weekly Report, Centers for Disease Control and Prevention, 2016. Retrieved from: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6450a3.htm.
15. Christopher M. Jones, Joseph Logan, Matthew R. Gladden, and Michele K. Bohm, “Vital signs: Demographic and substance use trends among heroin users—United States, 2002-2003.” Morbidity and Mortality Weekly Report, Centers for Disease Control and Prevention, 2016. Retrieved from: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6426a3.htm.
16. “Increases in drug and opioid overdose deaths—United states, 2000- 2014.” Centers for Disease Control and Prevention. Retrieved from: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6450a3.htm.
17. Lindsey Cook, “The heroin epidemic, in 9 graphs,” US News and World Report, August 19, 2015. Retrieved from: http://www.usnews.com/news/blogs/data-mine/2015/08/19/the-heroin-epidemic-in-9-graphs.
18. T.J. Cicero, M.S. Ellis, H.L. Surratt, and S.P. Kurtz, “The changing face of heroin use in the United States: A retrospective analysis of the past 50 years.” JAMA Psychiatry, 71(2014): 821-826.
19. See http://www.cdc.gov/drugoverdose/data/statedeaths.html.
20. See https://www.drugabuse.gov/about-nida/legislative-activities/testimony-to-congress/2016/americas-addiction-to-opioids-heroin-prescription-drug-abuse.
21. Shane Darke, “Pathways to heroin dependence: Time to re-appraise selfmedication,” Addiction, 108(2012), 659-667; Karolina M. Bogdanowicz, Robert Stewart, Matthew Broadbent, Stephani L. Hatch, Matthew Hotopf, John Strang, and Richard D. Hayes, “Double trouble: Psychiatric comorbidity and opioid addiction—All-cause and cause-specific mortality,” Drug and Alcohol Dependence, 148(2015), 85-92.
22. Lisa W. Foderaro, “Ithaca’s antiheroin plan: Open a site to shoot heroin,” The New York Times, March 22, 2016. Retrieved from: http://www.nytimes.com/2016/03/23/nyregion/fighting-heroin-ithaca-looks-to-injection-centers.html.
23. For a graphic illustrating use of illicit drugs by age, see http://bakerinstitute.org/media/cached/files/10688/700x525/Sub3-PastMonth.jpg.jpg.
24. William Martin and Jerry Epstein, “Rx for U.S. Drug Policy: A New Paradigm.” Baker Institute Policy Report Number 63, 2015, http://bakerinstitute.org/research/rx-us-drug-policy-new-paradigm/.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


