
Abstract
The Affordable Care Act and changing economic conditions have encouraged an increase in the integration of physicians with hospitals. Current research has focused on the overall trend of tighter integration, but it has not examined the more granular level of how hospitals transition between integration levels.
The objective of the study is to examine trends in physician-hospital integration over time. We used the 2008-2013 American Hospital Association annual survey data to designate four forms of integration based on the type of contractual relationship a hospital has with physicians. We examined overall changes in the number and percentage of hospitals engaged in varying forms of physician-hospital integration and the transitions between these integration levels by hospitals over time.
Between 2008 and 2013, the share of hospitals with physicians on salary rose from 44 to 55 percent of all facilities. Looser forms of physician-hospital integration, such as joint contractual networks with managed care organizations, decreased in prominence. However, the aggregate shift toward tighter vertical integration masks the fact that many hospitals de-integrated or shifted to less tightly integrated physician-hospital relationships during this time period.
The shift to tighter physician-hospital integration is more complex than previously expected. Future studies that distinguish between integration types are essential for setting policies that foster integrated care to improve quality and lower costs, instead of raising prices and harming patient welfare.
Introduction
The Affordable Care Act (ACA) and changing economic conditions have encouraged an increase in physician-hospital integration. In particular, Accountable Care Organizations (ACOs) and medical homes will continue to spur integration over the coming years. Policy experts and clinicians have described the potential of ACOs to improve health care quality and control cost growth.1, 2, 3, 4
In general, health care is shifting from volume-based to value-based; and the measure of success is correspondingly making a shift toward the ability to provide high quality outcomes and access to care for the lowest cost.5 Through integration hospitals could better control physician practices to increase efficiency and decrease costs.6 Increased integration could reduce duplication of services, provide clinical benefits, and improve communication and coordination of care between hospitals and physicians.7 A growing number of hospitals are employing not only hospitalists, but also primary and specialty care doctors. A 2010 survey showed that in the next 12 to 36 months 74 percent of hospital leaders planned to employ a greater percentage of physicians, and over 71 percent had received more requests than normal from physician groups for employment.8 A 2007–2008 American Medical Association (AMA) survey found that 16.3 percent of physicians worked in direct hospital employment or employment in a hospital-owned practice.9 In 2012, 29 percent of physicians worked directly for a hospital (5.6 percent) or for a practice that was at least partially owned by a hospital (23.4 percent).10 Current research has focused on the overall trend of tighter integration, but it has not examined at the more granular level how hospitals transition between integration levels. And contrary to the increase in integration that is generally discussed in the literature, many hospitals are de-integrating or shifting to less tightly integrated physician-hospital relationships.
This analysis reports (1) overall changes in the number and percentage of hospitals in varying forms of physician-hospital integration and (2) the transitions between these integration levels by hospitals from 2008 to 2013. Our data show an overall trend of increasing integration, yet there are also many hospitals transitioning to lower levels of physician-hospital integration.
Methods
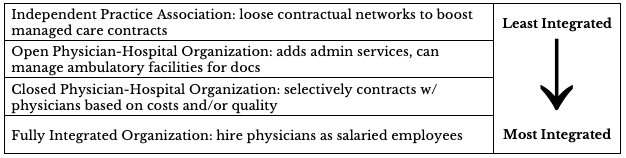
To define physician-hospital integration, we focused on general medical and surgical hospitals (as designated by AHA) and the differing levels of contractual control they may have with physicians. Based on previous literature, we used the AHA annual survey data to designate four forms of integration listed in Table 1: independent practice associations (IPA), open physician-hospital organizations (OPHO), closed physician-hospital organizations (also including the highly similar management services organizations) (CPHO), and fully integrated organizations (including both integrated salary model and foundation hospitals) (FIO).11, 12, 13 The AHA asked hospitals to identify the type of arrangement they establish with physicians. If a hospital claimed more than one integration type, then they were classified using the most integrated form reported.14 If a hospital reported a change in one year and a return to the previous form in the following year, then the hospital was assigned the original integration level for all three years (e.g., a hospital with survey responses of IPA in 2008, none in 2009, and IPA in 2010 would be assigned the value of IPA for 2008-2010).
IPAs are the loosest form of integration; in this form, a contractual network primarily provides services to boost managed care. The hospital provides physicians with few services but may assist physicians in contracting with managed care plans. This loose affiliation may boost demand for the hospital, increasing its market power. The OPHO invites all physicians in the market to join a management organization, which facilitates contracting with health plans and provides administrative services; this form of integration has equal capitalization and ownership between medical staff and the hospital. The CPHO is similar, except it selects physicians on the basis of cost, quality, or both.15 Physicians participating in CPHOs generally do not enter into similar agreements with other hospitals, although they may maintain admitting privileges in other hospitals.16 The tightest form of integration, the FIO, hires physicians as salaried employees and owns the practice.17
Table 1 — Physician-Hospital Integration Explanatory Variable Definitions
Results
Overall Trends in Physician-hospital Integration
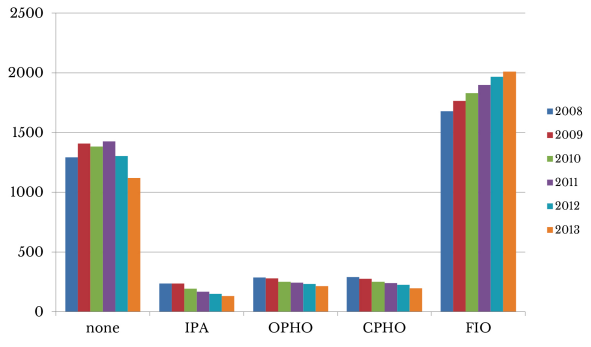
We measured the change in integration over time using AHA annual survey data for the years 2008-2013. In any given year, 24 to 29 percent of hospitals had no response to the survey question on integration type and were omitted from the analysis. As Figure 1 illustrates, most hospitals reported no integration with physicians, or that they were fully integrated facilities. The number of hospitals with looser forms of integration (IPA, OPHO, and CPHO) was much lower and declined over the years studied; the greatest change was an overall decrease of 107 hospitals classified as IPAs between 2008 and 2013. The total number of hospitals in the most tightly integrated form, FIO, increased by 332 over this time frame.
Figure 1 — The Number of Hospitals by Level of Integration* With Physicians Over Time
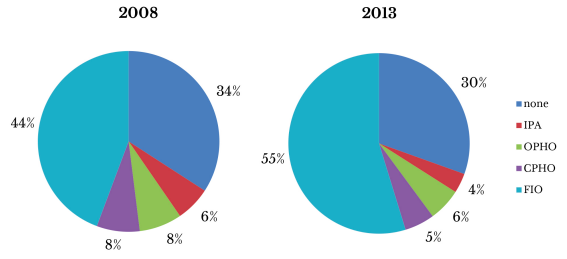
Since the number of hospitals participating in the AHA survey dropped from 3,787 in 2008 to 3,672 in 2013, we examined the share of hospitals in each category of integration in addition to the level of integration. Like Figure 1, Figure 2 illustrates a corresponding decrease in the percent of hospitals with looser forms of integration (IPA, OPHO, and CPHO) over the years studied, with the greatest change being a 2.8 percentage point decrease in the portion of hospitals classified as an IPA. The percentage in the most tightly integrated form, FIO, increased over this time frame, with 55 percent of hospitals fully integrated in 2013, 10 percentage points higher than in 2008. The patterns in the number and percent of physician-hospital agreements suggest that hospitals and physicians are creating new—or moving toward tighter—forms of integration.
Figure 2 — The Percentage of Hospitals by Level of Integration* With Physicians Over Time
Transitions in Physician-Hospital Integration by Hospital
Table 2 examines the changes in integration more closely by identifying the transitions in physician-hospital integration by hospital from 2008 to 2013. There are 4,727 hospitals represented by 23,966 hospital-year observations in the data. Some hospitals transitioned more than once in the six-year period, resulting in more total transitions than there are individual hospitals that transitioned. In all, there are 1,525 hospital-year observations reflecting a change in the integration level of 1,445 hospitals between 2008 and 2013. The remaining 3,282 hospitals maintained the same level of integration throughout the sample period.
Table 2 — Physician-Hospital Integration Level* Transition Matrix 2008–2013
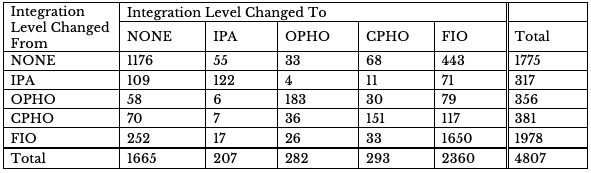
There are 599 cases in which a hospital switched from no integration to some level of integration between years. The level of integration with the greatest change is the fully integrated hospitals category, with 710 transitions to FIO agreements. A majority of this growth comes from the 550 hospitals changing from no integration to a FIO. An additional 156 hospitals established some other type of integration (IPA, OPHO, or CPHO) over the time period where there was none previously. There were 312 transitions from one form of integration to another tighter form of integration.
While there was a large transition to higher integration, many hospitals also transitioned from more tightly to less integrated forms of physician arrangements. In fact, hospitals with an IPA were almost as likely to transition to no integration as to remain as IPAs. Although the net change in hospital-year observations with no physician-hospital integration was only a decrease of 110, there were 489 hospital-year transitions that reflect de-integration across this time period. About half of these hospital-year observations transitioned from FIO to no integration. There are 125 observations that showed a change from an existing form of integration to one that was looser.
Discussion
The review of hospital integration data from 2008 to 2013 confirms the expected overall shift toward more tightly integrated physician-hospital arrangements. But when the individual hospital changes in integration are examined, it is apparent that this shift is not one-way. Many hospitals increased or decreased their level of integration — or seesawed between increasing and decreasing integration — over the period studied. The data suggest that the observed overall shift to tighter physician-hospital integration does not have a consistent pattern and may be more complex than previously expected.
Causes of Changes in Integration
Conflicting interests play a role in the choice to integrate or de-integrate.18 The trends in physician employment by hospitals between 2008 and 2013 were influenced by a variety of factors, including the desire to gain greater control of referrals from key specialists, as well as preparing for value- based contracting.19 During this time, Medicare reimbursement rates for specialties such as cardiology, orthopedic surgery, and related imaging services began declining.20, 21, 22 Such specialists were attractive to hospitals because they generated significant patient volume. Still, hospitals were uncertain about the physicians they should employ: highly compensated specialists or primary care physicians.
For their part, specialists saw the risk of declining incomes and sought partnerships with hospitals, where reimbursements for ancillary services previously provided in private practice were paid at higher levels when billed as the service of a hospital provider organization.23
It is fair to say that between 2008 and 2013, the optimal direction for hospital-physician integration was not clear for either hospitals or physicians. Pivots between strategies likely led to some de-integration.
The issue was compounded by the complex nature of physician integration strategies. A successful partnership requires physicians and hospitals to have aligned goals and strategies consistent across the organization; both the cultural fit and financial considerations of physicians and hospitals must be considered when weighing the decision to integrate.24, 25 In other words, when physicians seek hospital employment, they may expect little change in the way their businesses operate. But the expectation of their new employer—the hospital—is for physicians to maintain their pre-employment productivity; operate their clinics in alignment with hospital systems, processes, and policies; and more tightly align referrals with the hospital’s medical staff and outpatient services. When physician and hospital expectations are not clearly defined and aligned, the relationship may not achieve the desired results for either party. In such cases, the partnership has a high likelihood of failure.
The vast differences in culture between physician practices and hospitals can make the alignment of goals difficult. Physician practices operate as small businesses, with family members holding key staff positions, easy decision-making processes, simple supporting technologies, and tight budgets, while hospitals function as larger, more sophisticated business entities. Shifts in decision-making authority, transparency, EMR/practice management systems, and HR policies affecting practice staff are among the major changes physicians face after integrating with a hospital. For example, nurses’ payment policies and scheduling may be altered to match the hospital’s standardized system. Physicians and their staffs should be well prepared to anticipate these and other changes, and the hospital should be clear on which functions require standardization and which physicians will be allowed to control.
Other potential stumbling blocks to integrating a hospital and an independent physician practice involve payer contracting for Part B services; coding, billing, and collections processes and related technologies; staffing costs, policies and procedures; and supply chain management. All operate differently in a physician’s office as compared to a hospital. For example, supply costs under a hospital will be negotiated in a manner such that there are lower costs for the supplies needed by a hospital, but the mix of supplies required for clinic care may be quite different. Therefore, clinic operation costs may rise post-integration, leading the hospital to pressure physicians to restrain costs or de-integrate as financial losses mount.
To avoid such a situation, it is crucial for hospitals to create an effective governance structure that includes strong physician leadership and experienced practice administrators who assimilate and galvanize once-independent groups with the hospital’s developing infrastructure. Hospitals must put a leadership team in place with experience in this space to support clinic operations, lest physician discontent and distrust increase, causing an integration strategy to spiral down and end in de-integration.26 It is possible that hospitals unable to control costs, increase quality, or sustain price increases may have chosen to deintegrate in the period studied.27, 28
As time progressed, more regulations associated with the Affordable Care Act have been rolled out offering various payment innovations and new opportunities for both physicians and hospitals to participate in value-based contracting. These options provided better solutions with less operating and financial risk for hospitals and physicians, and may have led both parties to go their separate ways. For example, hospitals have relied on the strength of their relationships with clinically integrated IPAs to form successful accountable care organizations (ACOs), allowing physicians to retain their private practices yet still benefit from the shared savings they produce.29 Yet the growth in public and private ACOs has likely increased the desire of hospitals and physicians to forge FIOs in order to deliver coordinated care that achieves cost savings that are commonly awarded under ACO contracts. The Medicare program attributes patients to an ACO based on their most frequently visited primary care physician (PCP). Thus, a hospital seeking to participate as a Medicare ACO must build relationships with these PCPs and will have better control of hospital referrals for inpatient and outpatient care if these PCPs are hospital employees. Physician groups that lacked the financial and technical expertise to adopt electronic health records that have increasingly become necessary to obtain higher reimbursements by public and private payers may have been most attracted to FIOs.
Other organizations seeking an alternative to tighter integration have contracted with newly forming national practice management service organizations like Privia and Evolent to organize and provide supporting population health management infrastructure such as technology, data management and monitoring, care coordination, and patient workflow for their physician partners in pursuing value based contracts.30, 31
Effects of Changes in Integration
Previous literature offers inconsistent conclusions about the effects of physician-hospital integration. Some studies suggest that tighter levels of physician-hospital integration may be associated with higher expenditures.32, 33, 34 There is limited, mixed evidence of the effect of integration on admissions and utilization.35, 36 Evidence on the association between integration and quality of care is similarly contradictory. While several studies show quality improvements when physicians and hospitals are integrated, others reveal lower quality or no association between integration and quality measures.37, 38, 39, 40, 41, 42 Additionally, most previous research suggests that physician-hospital integration may increase the price of health care.10–12,3043, 44, 45, 46
We believe the AHA survey data reflect a genuine signal about integration trends in the aggregate because the trend of increasing vertical integration is corroborated by independent research using other data sources.47, 48, 49 However, given the self-reported nature of the AHA survey, some of the variability from year to year—which is highlighted in this analysis—may not be meaningful.
Future studies should distinguish between different physician-hospital integration types, and how each type affects expenditures, utilization, and prices. Loose forms of integration that generate more managed care contracts and provide administrative services could increase utilization and expenditures, with no improvement in quality or lower costs. Achieving these latter two goals is likely only with tighter integration, which has features similar to those of ACOs and medical homes. Further analyses are essential for setting policies that foster integrated care that improves quality and lowers costs, instead of raising prices and harming patient welfare.
Endnotes
1. E.S. Fisher et al., “Fostering Accountable Health Care: Moving Forward in Medicare,” Health Affairs 28, no. 2 (2009): 219–231, doi:10.1377/hlthaff.28.2.w219.
2. F. Mostashari and J.A. Colbert, “Four Key Competencies for Physician-led Accountable Care Organizations, American Journal of Accountable Care 3 (2014): 15–16.
3. F.J. Crosson, “The accountable care organization: Whatever its growing pains, the concept is too vitally important to fail,” Health Affairs 30, no. 7 (2011): 1250–1255, doi:10.1377/hlthaff.2011.0272.
4. S. DeVore and R.W. Champion, “Driving population health through accountable care organizations,” Health Affairs 30, no. 1 (2011): 41–50, doi:10.1377/hlthaff.2010.0935.
5. M.T. Flores, “Physician Integration in a Value-Based Era,” Hospital and Health Networks, 2012. Available at: http://www.hhnmag.com/articles/6192-physician-integration-in-a-value-based-era. Accessed April 7, 2016.
6. L. Summer, Integration, Concentration, and Competition in the Provider Marketplace, 2010. Available at: http://www.academyhealth.org/files/publications/ AH_R_Integration FINAL2.pdf. Accessed April 13, 2015.
7. Ibid.
8. J. Cantlupe, Physician Alignment in an Era of Change, 2010. Available at: http://uconnhealth2020.uchc.edu/knowledgebase/pdfs/healthcare_reform/physician_ alignment_era_change.pdf.
9. C. Kane, The Practice Arrangements of Patient Care Physicians, 2007-2008: An Analysis by Age Cohort and Gender, 2009. Available at: http://www.amaassn.org/ama/pub/advocacy/health-policy/policy-research.page.
10. C. Kane and D. Emmons, New Data On Physician Practice Arrangements: Private Practice Remains Strong Despite Shifts Toward Hospital Employment, 2013. Available at: http://www.ama-assn.org/ama/pub/advocacy/health-policy/policy-research.page.
11. L.C. Baker, M.K. Bundorf, and D.P. Kessler, “Vertical Integration: Hospital Ownership Of Physician Practices Is Associated With Higher Prices And Spending,” Health Affairs 33, no. 5 (2014): 756–763, doi:10.1377/hlthaff.2013.1279.
12. F. Ciliberto and D. Dranove, “The effect of physician-hospital affiliations on hospital prices in California,” Journal of Health Economics 25, no. 1 (2006): 29–38, doi:10.1016/j.jhealeco.2005.04.008.
13. A.E. Cuellar and P.J. Gertler, “Strategic integration of hospitals and physicians,” Journal of Health Economics 25, no. 1 (2006): 1–28, doi:10.1016/j.jhealeco.2005.04.009.
14. Baker, “Vertical Integration,” Health Affairs, 2014.
15. M. Brown, Integrated Health Care Delivery: Theory, Practice, Evaluation, and Prognosis, Aspen Publishers, Inc., 1996. Available at: http://books.google.com/books/about/ Integrated_Health_Care_Delivery.html?id=E9bFfb5yp80C&pgis=1. Accessed April 13, 2015.
16. Baker, “Vertical Integration,” Health Affairs, 2014.
17. Ibid.
18. D. Burda, “The hard path of physician integration,” Moderm Healthcare, 2011. Available at: http://www.modernhealthcare.com/article/20110323/NEWS/110329980. Accessed April 4, 2016.
19. G. Aston, “Hospitals Wise Up When Adding Physician Practices,” Hospital and Health Networks, 2013. Available at: http://www.hhnmag.com/articles/5993-hospitals-wiseup-when-adding-physician-practices. Accessed April 13, 2016.
20. J. Nordt, M. Connair, and J.A. Gregorian, As Medicare Costs Rise, Reimbursements Drop, American Academy of Orthopaedic Surgeons. Available at: http://www.aaos.org/AAOSNow/2012/Dec/cover/cover1/?ssopc=1.
21. J. Helm, Surprisingly Common Trends in Cardiology Physician Compensation, VMG Health. Available at: http://www.vmghealth.com/Downloads/ SurprisinglyCommonTrendsinCardiologyPhysicianCompensation.pdf. Accessed November 10, 2016.
22. D.C. Levin et al., “The sharp reductions in medicare payments for noninvasive diagnostic imaging in recent years: Will they satisfy the federal policymakers?” Journal of the American College of Radiology 9, no. 9 (2012): 643–647, doi:10.1016/j.jacr.2012.05.004.
23. S. Baltic, “Monopolizing medicine : Why hospital consolidation may increase healthcare costs,” Medical Economics, February 24, 2014. Available at: http://medicaleconomics.modernmedicine.com/medical-economics/content/tags/hospital-employment/monopolizing-medicine-why-hospital-consolidation-.
24. S. Hoppszallern, “Physician Integration Strategies in a Rural Network,” Hospital and Health Networks, 2012. Available at: http://www.hhnmag.com/articles/5505-physician-integration-strategies-in-a-rural-network. Accessed April 14, 2016.
25. Aston, “Hospitals Wise Up,” Hospital and Health Networks, 2013.
26. Ibid.
27. Ciliberto, “The effect of physician-hospital affiliations,” Journal of Health Economics, 2006.
28. B. Kutscher, “Making physicians pay off: Hospitals struggle to balance current costs with future benefits of employing docs,” Modern Healthcare, 2014. Available at: http://www.modernhealthcare.com/article/20140222/MAGAZINE/302229986.
29. Baltic, “Monopolizing medicine,” Medical Economics, 2014.
30. Privia Health. Available at: http://www.priviahealth.com/. Accessed October 19, 2016.
31. Evolent Health. Available at: https://www.evolenthealth.com/our-solutions/overview. Accessed October 16, 2016.
32. K. Madison, “Hospital-physician affiliations and patient treatments, expenditures, and outcomes,” Health Services Research Journal 39, no. 2 (2004): 257–78, doi:10.1111/j.1475-6773.2004.00227.x.
33. J.C. Robinson and K. Miller, “Total expenditures per patient in hospital-owned and physician-owned physician organizations in California,” Journal of the American Medical Association 312, no. 16 (2014): 1663–9, doi:10.1001/jama.2014.14072.
34. Baker, “Vertical Integration,” Health Affairs, 2014.
35. Ibid.
36. Madison, “Hospital-physician affiliations,” Health Services Research Journal, 2004.
37. Ibid.
38. J. Stensland and T. Stinson, “Successful Physician-Hospital Integration in Rural Areas,” Medical Care 40, no. 10 (2002): 908–917, doi:10.1097/00005650-200210000-00008.
39. C.S. Carlin, B. Dowd, and R. Feldman, “Changes in Quality of Health Care Delivery after Vertical Integration,” Health Services Research Journal 2015: 1043–1069, doi:10.1111/1475-6773.12274.
40. A. Chukmaitov et al., “Delivery system characteristics and their association with quality and costs of care: Implications for accountable care organizations,” Health Care Management Review 40, no. 2. (2015): 92–103, doi:10.1097/HMR.0000000000000014.
41. S.M. Shortell et al., “An Empirical Assessment of High-Performing Medical Groups: Results from a National Study,” Medical Care Research Review 62, no. 4 (2005): 407– 434, doi:10.1177/1077558705277389.
42. Cuellar, “Strategic integration,” Journal of Health Economics, 2006.
43. Ibid.
44. Baker, “Vertical Integration,” Health Affairs, 2014.
45. Ciliberto, “The effect of physician-hospital affiliations,” Journal of Health Economics, 2006.
46. R.A. Berenson, P.B. Ginsburg, and N. Kemper, “Unchecked provider clout in California foreshadows challenges to health reform,” Health Affairs (Millwood) 29, no. 4 (2010): 699–705, doi:10.1377/hlthaff.2009.0715.
47. Cantlupe, Physician Alignment, 2010.
48. Kane, Practice Arrangements, 2009.
49. Kane, New Data On Physician Practice Arrangements, 2013.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


