
To access the Spanish version of this policy brief, download the PDF on the left-hand sidebar.
Abstract
West Nile, dengue, and chikungunya are all caused by arthropod-borne viruses (arboviruses), which are transmitted primarily via mosquitos. In total, they result in more than 100,000 annual infections in the United States and Mexico. This number is predicted to increase as the mosquito populations carrying arboviruses move northward due to climate change and general migration of the mosquitos and infected individuals. Unlike other neglected tropical diseases (NTDs) that are more common in rural areas, these arboviruses are often found in poor urban areas as well as suburbs and more affluent neighborhoods. Despite the increasing risks in the United States and Mexico, policymakers have made little effort to prevent future outbreaks. The US and Mexican governments should collaborate towards comprehensive vector control programs and awareness campaigns for these mosquito-transmitted diseases. Furthermore, additional research on preventative measures, including the development of vaccines, would dramatically limit the spread of these debilitating diseases.
Background
Arboviruses are a class of viruses which are transmitted via mosquitos or other insect vectors. Dengue (DENV), chikungunya (CHIKV), and West Nile virus (WNV) all have recently emerged and created widespread epidemics in Mexico and the United States. While each disease is caused by a different virus and causes different symptoms in affected patients, they are commonly categorized together since preventative and public health measures to contain them overlap considerably.
WNV and DENV are both caused by viruses belonging to the flavivirus family, while CHIKV is a type of alphavirus (Lo Presti 2014; Amanna 2014). All three utilize single-stranded RNA for genomic information and replication, rather than double-stranded DNA, which is present in humans. While all three arboviruses are predominantly transmitted via mosquitos, they can also be transmitted through blood transfusions and organ donations as well as congenital transmission from mother to fetus (Centers for Disease Control and Prevention–WNV, DENV, CHIKV).
Figure 1 — Dengue, Chikungunya and West Nile Viruses
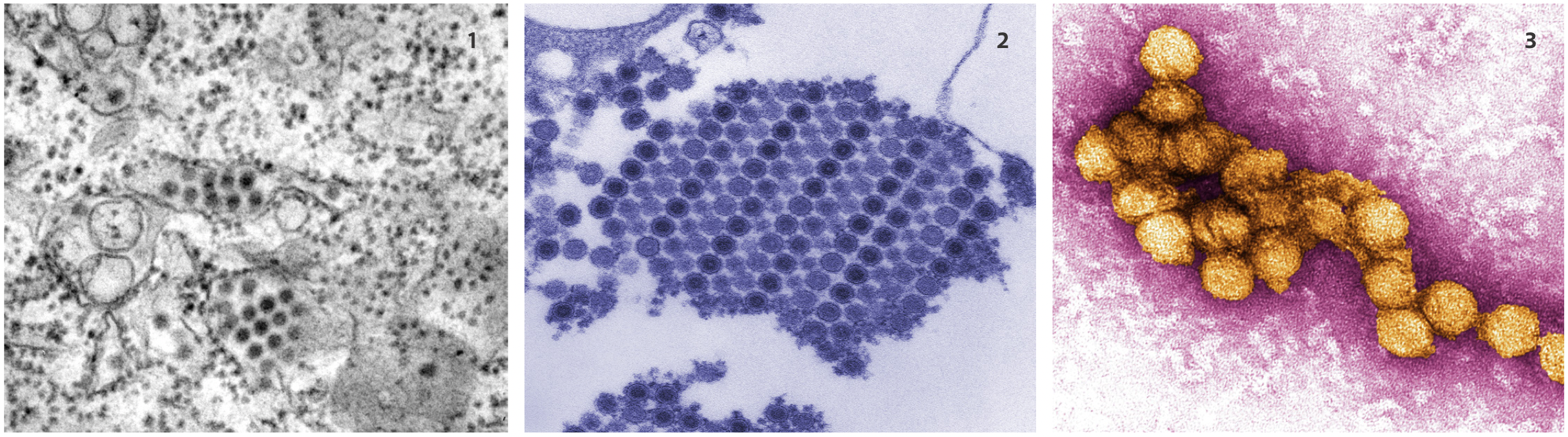
WNV has been described in three distinct stages of infection: the initial infection or early stage, the virus amplification stage, and the neuroinvasive stage (Suthar and Pulendran 2014). In the early stage, after infection, the WNV replicates in the skin cells at the site of the mosquito bite. The virus then moves to the spleen and other peripheral organs such as the liver and kidney where it amplifies further. In the final and less common stage, the virus enters the central nervous system. While most cases of WNV are asymptomatic, approximately 25 percent of patients present with West Nile fever. Symptoms of West Nile fever include high fever, general fatigue, headache, and body aches (Amanna 2014; CDC-WNV). Less than 1 percent of infected individuals develop the more severe West Nile neuroinvasive disease, which can cause encephalitis or meningitis, characterized by inflammation of the brain or surrounding membranes (CDC-WNV). In addition, even mild cases of WNV can have long-term consequences and have recently been linked to chronic kidney disease and renal failure (Patel, Sander and Nelder 2015; Murray et al. 2014; Nolan et al. 2012). At this time, there are no vaccines available to prevent disease nor specific antiviral to treat clinical infection.
DENV infection is distinctly different from WNV infection, even though both are caused by flaviviruses. DENV has four distinct serotypes (DENV 1, 2, 3, and 4), and infection with each serotype results in a similar clinical presentation. After an infected mosquito bites a human, the DENV migrates to the lymph nodes then through the bloodstream to the entire body (CDC-DENV). Symptoms usually occur four to seven days after the initial infection and can include a high fever; severe headache; severe pain behind the eyes; joint, muscle, or bone pain; a rash; mild bleeding (from the nose or gums); and easy bruising (CDC-DENV). The pain can often be so intense that the term “breakbone fever” is commonly used to describe DENV infection. In some cases, dengue hemorrhagic fever (DHF) can develop three to seven days after the initial symptoms of dengue fever appear. This clinical manifestation is more likely to occur when an individual has a prior history of DENV infection with a different serotype (i.e., infected with DENV serotype 1, then years later becomes infected with DENV serotype 2). Initially, the patient with DHF will present symptoms compatible with dengue fever for two to seven days. However, after the fever begins to decline and the patient begins to show signs of improvement, additional symptoms develop, including severe abdominal pain, persistent vomiting, and difficulty breathing (CDC-DENV).
A hallmark feature of DHF is plasma leakage, which is when the liquid component of the blood (or plasma) leaks out of capillaries and other blood vessels (CDC-DENV) and causes bleeding under the skin and internally. The patient’s condition can continue to deteriorate into dengue shock syndrome (DSS), characterized by dangerously low blood pressure. If left untreated, DHF and DSS can be fatal, although the mortality rate is only 1 percent when appropriate and aggressive medical care is administered. To continue the cycle of infection, the mosquito obtains the DENV from an infected human during feeding, and after eight to 12 days of incubation, the mosquito can pass along the virus to the next host for the remainder of its life (CDC-DENV). The clinical attack rate for DENV is high, with 80 percent to 90 percent of people bitten by infected mosquitos developing the disease.1 At this time, there are no vaccines available to prevent disease and no specific antiviral to treat clinical infection.
The disease name chikungunya is a Makonde2 word meaning “that which bends up,” referring to the posture of affected patients with severe joint pain (Lo Presti 2014). Following the initial infection, CHIKV replicates first in the skin, then spreads through the blood to the liver, muscles, joints, spleen, lymph nodes, and brain (Lo Presti 2014). CHIKV symptoms usually develop three to seven days after the initial mosquito bite and are similar to dengue symptoms, including high fever, headache, photophobia, rash, and joint swelling with severe pain (CDC-CHIKV; Lo Presti 2014). Ninety-five percent of infected adults develop symptoms and most suffer from decreased mobility and dexterity that can cause disability for months to years following infection (Thiboutot et al. 2010). As with the case of WNV and DENV, there are no vaccines available to prevent disease from CHIKV and no specific antiviral to treat clinical infection.
Young children and the elderly are more susceptible to developing the more severe symptoms of WNV, CHIKV, and DENV (CDC-CHIKV, DENV, WNV). Initial infections are usually asymptomatic and are difficult to detect until the disease becomes clinically apparent. A blood test can detect the viruses in patients who show symptoms, but there are no specific treatments for WNV, DENV, and CHIKV other than supportive care. Most interventions merely treat the symptoms with generic medications such as ibuprofen and acetaminophen to relieve fever and pain (CDC-CHIKV, DENV, WNV). Patients are also encouraged to rest and stay hydrated during the duration of their illnesses.
Disease Rates and Distribution
Of the three arboviruses discussed, WNV is the most commonly known and most geographically widespread (Amanna 2014). In addition to mosquito migration, WNV has also been linked to the migration of birds across North America (Elizondo-Quironga 2013). Birds are the reservoir host for WNV, meaning they amplify high enough levels of the virus in the blood to cause mosquitos to become infected at the time of the blood meal. WNV first appeared in the United States in New York in 1999. Since then, it has spread across the country. As of January 2015, WNV infection has resulted in more than 41,000 human cases and 1,700 deaths throughout the United States.3 In 2014, the United States had 2,205 reported cases of WNV and 97 deaths (Table 1). The top three ranking states with WNV infections include California (801 cases), Texas (379 cases), and Nebraska (142 cases).
The economic burden of WNV on a community can be great. In 2012, Texas experienced its largest WNV outbreak to date, resulting in 1,868 clinical infections, including 844 cases of West Nile neuroinvasive disease and 89 deaths. Minority populations were at greatest risk for being diagnosed with neuroinvasive disease (Murray et al. 2013). The most likely reason for this is that minority populations have less access to medical care, leading to unreported cases and deceptively lower numbers of reported milder fever cases.4 The outbreak resulted in an estimated $47 million in acute care and lost productivity, not including long-term costs or mosquito control efforts. Interestingly, there has yet to be any outbreaks of WNV in Mexico or Latin America, with less than 20 cases of WNV reported in Mexico annually (Elizondo-Quironga 2013). The reason for this is unknown.
Table 1 — Cases (and Deaths) Associated With WNV, DENV and CHIKV in 2014
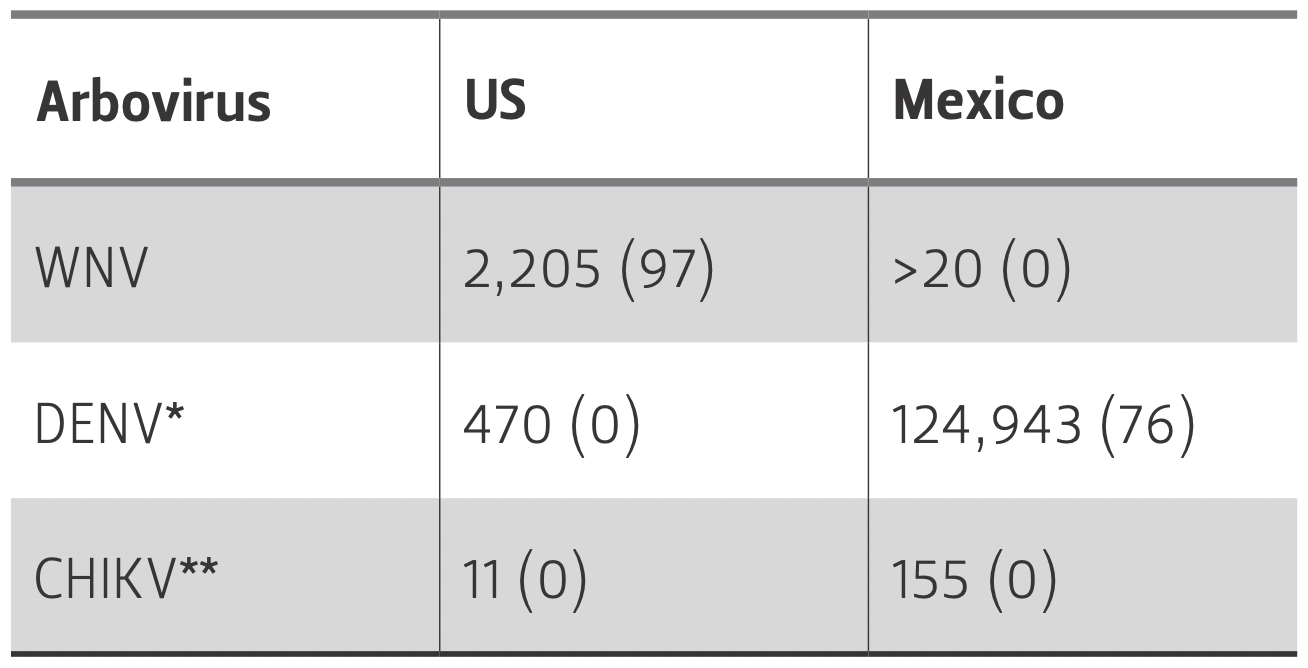
Source CDC; Pan American Health Organization; Darwin Elizondo-Quiroga and Armando Elizondo-Quiroga, 2013, "West Nile Virus and its theories, a big puzzle in Mexico and Latin America," Journal of Global Infectious Diseases.
DENV is believed to be the most rapidly spreading mosquito-borne viral disease in the world, with an estimated 50 million to 100 million annual infections and 2.5 billion people living in locations at risk for DENV (CDC-DENV; World Health Organization). Before 1970, only nine countries reported outbreaks of DENV, but by 2014, this number had increased to 128 countries in Africa, the Americas, Asia, Europe, and the Pacific—with a 30-fold increase in incidences (WHO). Outbreaks of DENV are not new to the United States. During the “Galveston outbreak” in 1922, Texas saw an estimated 500,000 cases.5 In 2014, there were 470 suspected cases of DENV in the United States reported to the Centers for Disease Control and Prevention (Table 1). That same year, the number of suspected cases in Mexico was significantly higher, with 124,943 reported cases and 76 disease-related deaths. In fact, DENV in Mexico is currently considered hyper-endemic, or having a high incidence of cases, with 28 out of the 32 Mexican states reporting DENV transmission (Undurraga 2015). The annual cost of DENV intervention in Mexico has been estimated at $170 million, with $83 million spent on vector control and surveillance (Undurraga 2015).
CHIKV outbreaks, once isolated to Africa before 1958, now have reached northern Mexico and threaten to spread into the United States and Mexico (Weaver 2015). More than 1.25 million cases of CHIKV have been reported in the Americas since it first appeared in the Western Hemisphere in late 2013 (CDC-CHIKV). Between 2013 and 2014, only 11 cases of CHIKV were reported in the United States and 155 in Mexico (Table 1). That number increased dramatically in 2015, with more than 7,100 cases in Mexico6 and 114 imported cases in the state of Texas alone.7 The majority of CHIKV cases in the United States occurred in travelers returning from infected areas; however, local transmission has recently been reported in Florida (CDC-CHIKV). In addition, there is a high rate of CHIKV mosquito infection after a mosquito bites an infected human, which can lead to large populations of infected mosquitos and consequently can increase the incidence of infection in humans (Weaver 2015).
Risk and Prevention
Studies have linked arboviruses, especially WNV infection rates, with social and environmental factors. These include temperature, precipitation, land-use changes, urbanization, and socioeconomic factors such as income level and host biodiversity (Harrigan 2014). Climate change increases many of the environmental risks, leading to increased WNV as well as CHIKV and DENV incidence in North America.
As expected with transmission linked to mosquito exposure, the risk of contracting these viruses increases as exposure to the insects increases. The best measure to prevent arbovirus infection is to avoid mosquito bites. Individuals are encouraged to use insect repellants and avoid exposing skin when outside, as well as protect the home by utilizing mosquito nets or screens on open windows or doors and getting rid of standing water around the residence (CDC-CHIKV, DENV, WNV). These preventive measure can carry a high cost and may be unavailable to those living in poverty.
From a public health perspective, prevention involves controlling the insect vectors by spraying insecticides and removing standing water, where mosquitoes normally lay their eggs. Mexico has existing vector control programs through the Mexican Ministry of Health, which sprays indoor and outdoor insecticide to reduce or eliminate mosquito populations (Unduragga 2015). In the United States, vector control programs are organized at the local level (cities and counties) in communities where previous cases have existed (CDC-WNV). These programs are activated when arboviruses, most often WNV, are detected in the community to prevent further infections.
In addition to vector control or avoidance, researchers are actively pursuing vaccines on all three arboviruses. Vaccines exist for other flaviviruses—yellow fever, tick-borne encephalitis, and Japanese encephalitis viruses—but are not approved for DENV, CHIKV, or WNV (Flipse 2015). Overall, scientists are optimistic about their chances, in time, to develop WNV, DENV, and CHIKV vaccines. Several candidate vaccines are currently in clinical trials, but each virus has its own set of challenges. For example, because there are four serotypes of DENV, a tetravalent vaccine is required for effective intervention. Several veterinary vaccines for WNV previously have been developed, and work is ongoing for a human WNV vaccine (Amanna 2014). CHIKV vaccine research has also progressed slowly with several safety concerns (Tretyakova 2014).
Recommendations
Viruses and mosquitos do not acknowledge national boundaries, crossing from the United States to Mexico and back without regard to man-made or natural borders. In addition, international travelers are also bringing infections home with them, transferring these viruses to susceptible mosquito populations in the United States and Mexico. This potentially puts the local human populations at risk. Effective control of arboviruses requires both vector control polices as well as the development of effective vaccines to protect populations. To combat WNV, DENV, and CHIKV in the United States and Mexico, governments need to coordinate and collaborate to increase public awareness about risks and preventative measures as well as improve disease surveillance. Currently, the CDC works with the Mexican government through its Puerto Rico-based Dengue Branch and its US-Mexico Unit.8 These CDC divisions work with partners in Mexico, including the Mexican Secretariat of Health, to investigate infectious disease outbreaks and train public health workers on activities related to dengue surveillance and diagnosis.9 In addition to these efforts, both countries should devote additional resources towards vaccine development to prevent disease outbreaks in the future and protect public health.
Unfortunately, it may not be cost-effective to implement mass preventative measures such as vaccinations and mosquito spraying. Instead, targeted vaccination programs to communities in the United States and Mexico with past, current, or increased risk of future outbreaks would be more effective (Amanna 2014). However, the low incidence and sporadic nature of outbreaks in the United States, especially for CHIKV, makes finding an appropriate population to test vaccine efficacy difficult (Amanna 2014). But these challenges are not unique to arbovirus vaccines, as similar discussions regarding adequate and appropriate designs of clinical trials have been ongoing, most recently related to the testing of experimental Ebola treatments and vaccines.
In addition, vector control measures could inadvertently lead to increased infection rates by creating insecticide-resistant mosquito populations. Therefore, the best strategies would include active surveillance with local campaigns for vector control and, when available, vaccinations of at-risk populations once the viruses are detected in human, animal, or mosquito populations.
Mexico has taken the first step in ensuring successful vaccine introduction by convening a “Mexican Dengue Expert Group,” which consists of public health and public policy experts from the Mexican Federal Ministry of Health in partnership with the Carlos Slim Foundation (Betancourt-Cravioto et al. 2014). This group analyzed an array of issues, including disease tracking systems, economics, regulatory issues, communications, and immunization systems. As a result, a series of recommendations were developed and distributed to aid Mexico in the early adoption of a dengue vaccine. The United States should take a similar approach in preparing to introduce new technologies to address emerging diseases such as arboviruses.
Conclusion
Unlike many other NTDs, WNV, DENV, and CHIKV are not always associated with poverty and rural areas. In fact, WNV outbreaks in the United States have been found in urban as well as suburban settings. As our climate continues to change and models predict the migration of mosquitos capable of carrying these NTDs throughout the United States, adequate prevention and surveillance will be paramount. Regular surveillance for mosquito, animal, and human infections will be necessary in high-risk locations. This action will help public health officials mobilize to prevent wide-spread outbreaks. While current preventative measures focus on minimizing mosquito populations through spraying and eliminating mosquito breeding grounds, future efforts also should include vaccinations and antiviral therapies. Coordinated efforts between the United States and Mexico to achieve these goals will improve public health as well as build trust between our nations.
Endnotes
1. From remarks by Kristy Murray, DVM, Ph.D., associate professor at Baylor College of Medicine, at the Baker Institute conference, “The United States and Mexico: Addressing a Shared Legacy of Neglected
Tropical Diseases and Poverty,” September 29-30, 2015.
2. Makonde is spoken in Mozambique and Tanzania.
3. From remarks by Kristy Murray at the Baker Institute, September 2015.
4. Ibid.
5. Ibid.
6. From remarks by Mercedes Juan Lopez, MD, Mexico’s Secretary of Health, at the Baker Institute conference, “The United States and Mexico: Addressing a Shared Legacy of Neglected Tropical Diseases and Poverty,” September 29-30, 2015.
7. From remarks by Kristy Murray at the Baker Institute, September 2015.
8. From remarks by Dr. Mitchell I. Wolfe, MD, MPH, deputy assistant secretary, Department of Health and Human Services, at the Baker Institute conference, “The United States and Mexico: Addressing a Shared Legacy of Neglected Tropical Diseases and Poverty,” September 29-30, 2015.
9. Ibid.
References
Amanna Ian J. and Mark K. Slifka. 2014. “Current Trends in West Nile Virus Vaccine Development.” Expert Review of Vaccines. 13(5): 589-608. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4279923/.
Betancourt-Cravioto, Miguel, Pablo Kuri-Morales, Jesús Felipe González- Roldán, Roberto Tapia-Conyer, and the Mexican Dengue Expert Group. 2014. “Introducing a Dengue Vaccine to Mexico: Development of a Systme for Evidence-Based Public Policy Recommendations.” PloS Neglected Tropical Diseases 8(7): e3009.
Centers for Disease Control and Prevention (CDC). “Chikungunya Virus.” Retrieved from http://www.cdc.gov/Chikungunya.
CDC. “Dengue Homepage.” Retrieved from: http://www.cdc.gov/dengue.
CDC. “West Nile.” Retrieved from: http://www.cdc.gov/westnile. Elizondo-Quiroga, Darwin and Amando
Elizondo-Quiroga. 2013. “West Nile virus and its theories, a big puzzle in Mexico and Latin America.” Journal of Global Infectious Diseases 5(4): 168-175.
Flipse Jacky and Jolanda M. Smit. 2015. “The complexity of a dengue vaccine: A review of the human antibody response.” PloS Neglected Tropical Diseases 9(6): e0003749.
Harrigan, Ryan J., Henri A. Thomassen, Wolfgang Buermann, and Thomas B. Smith. 2014. “A continental risk assessment of West Nile virus under climate change.” Global Change Biology 20: 2417-2425.
Lo Presti, Alessandra, et al. 2014. “Chikungungya virus, epidemiology, clinics and phylogenesis: A review.” Asian Pacific Journal of Tropical Medicine 7(12): 925-32. http://www.sciencedirect.com/science/article/pii/S1995764514601644.
Murray, Kristy O., Duke Ruktanonchai, Dawn Hesalroad, Eric Fonken, and Melissa S. Nolan. 2013. “West Nile Virus, Texas, USA, 2012.” Emerging Infectious Diseases Journal 19(11): 1836-8. Murray, Kristy O., Melissa N. Garcia, Mohammad H. Rabhar, Diana Martinez, Salma A. Khuwaja, Raouf R. Arafat,
and Susan Rossmann. 2014. “Survival analysis, long-term outcomes, and percentage of recovery up to 8 years post-infection among the Houston West Nile virus cohort.” PLoS One 9: e102953.
Nolan, Melissa S., Amber S. Podoll, Anne M. Hause, Katherine M. Akers, Kevin W. Finkel, and Kristy O. Murray. 2012. “Prevalence of chronic kidney disease and progression of disease over time among patients enrolled in the Houston West Nile virus cohort.” PLoS One 7(7): e40374.
Patel, Hetal, Beate Sander, and Mark P. Nelder. 2015. “Long-term sequelae of West Nile virus-related illness: a systematic review.” The Lancet Infectious Diseases 15: 951-59.
Suthar, Mehul S. and Bali Pulendran. 2014. “Systems analysis of West Nile virus infection.” Current Opinion in Virology 6:70-75.
Thiboutot et al. 2010. “Chikungunya: A Potentially Emerging Epidemic?” PloS Neglected Tropical Diseases 4(4): e623. http://journals.plos.org/plosntds/article?id=10.1371/journal.pntd.0000623
Tretyakova, Irina, Jason Hearn, Eryu Wang, Scott Weaver, and Peter Pushko. 2014. “DNA Vaccine Initiates Replication of Live Attenuated Chikungunya Virus In Vitro and Elicits Protective Immune Response in Mice.” The Journal of Infectious Diseases 209(12): 1882-1890.
Undurraga, Eduardo A. et al. 2015. “Economic and Disease Burden of Dengue in Mexico” PloS Neglected Tropical Diseases 9(3): e0003547.
Weaver, Scott and Marc Lecuit. 2015. “Chikungunya Virus and the Global Spread of a Mosquito-Borne Disease.” The New England Journal of Medicine 372: 1231-1239.
World Health Organization (WHO). “Impact of Dengue.” Retrieved from: http://www.who.int/mediacentre/factsheets/fs117/en/.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


