
This brief is part of a series on the impact of Covid-19 on vulnerable families. The other reports focus on low-income mothers; undocumented immigrants; and resettled refugees in the U.S.
Introduction
The Covid-19 pandemic has illuminated the fragility of American life, with the stock market in turmoil, high unemployment rates, supply chain shortages, and excessive hoarding of everyday goods. Even as states reopen, people are still adjusting to a new way of daily life. For many families, stressors that were manageable before the pandemic are now exacerbated. They are worried about becoming ill, and their financial stability and security. Children are at home for extended periods of time, while parents try to manage work demands, provide support for their children, and cope with rapidly changing circumstances. Pre-existing stressors, such as housing and food insecurity, marital discord, and dysfunctional parent-child relationships, are magnified; supportive measures to mitigate the impact of these stressors on mental and physical heath are difficult to access with social distancing measures in place. Covid-19 has accentuated many of the challenges that children, families and communities had been confronting, upsetting any balance that existed prior to the pandemic.
Brain Development
For young children, the effects of the pandemic have the potential for long-lasting negative impacts. Decades of research and developmental biology demonstrate that the first few years of life are critical for brain development.1 During this time, the foundational architecture of the brain is built in a hierarchal fashion through neuronal connections that occur at a rate of one million new connections per second.2 External stimuli drive which connections are strengthened and which die off, ultimately determining the strength of the overall architecture of the brain.3 Strong brain architecture is important for self-regulation, cognition, language, and many other social- and health-related functions.4 One of the most important external stimuli is parental or caregiver responsiveness to the child.5 Young children require lots of warm, loving interactions with caregivers. These positive interactions drive optimal brain development and a paucity of such interactions lead to suboptimal brain development.
Many vulnerable children and families exist in a delicate balance between daily challenges (poverty, mental illness, substance use, undereducation, structural injustices) and resilience forces (social capital, mental hardiness, community abundance). Anything that upsets this fragile balance (natural disaster, financial crisis) can result in profound child, family, and community distress. For example, disrupted parent-child interactions are more common during natural disasters in part because children express their anxieties and concerns differently than adults during these events, and adults may misinterpret those expressions as misbehavior.6 A child’s distress about the pandemic may manifest in a wide variety of different ways, including becoming “clingy,” uncharacteristic tantrums or outbursts, changes in sleep or appetite, or decreased interest in or engagement with typically enjoyed behaviors. Parents are also dealing with additional stressors and are more likely to respond harshly when stressed.7 Moreover, social isolation and economic losses can compound pre-existing mental health fragilities, causing impaired parent-child interactions.
The normal physiologic response to stress includes the release of cortisol (the “stress hormone”). While cortisol has many actions, one of its most clearly articulated effects is to slow neuronal growth. Thus, a growing infant brain that is subjected to persistent negative stress may be bathed in high levels of cortisol. This “toxic stress” has been demonstrated to result in anatomic and functional alteration in the growing brain.8 The growing brain is so dependent on external stimuli for its development that neurons that are not stimulated die, which can cause long-term cognitive and emotional deficits in a child. For example, a study of Romanian children who lived in an orphanage found that infants who were only changed, bathed, and fed, but who did not receive love, affection, or nurturing, had a severe deficit of brain volume of both gray matter, which is composed of neuronal cell bodies, and white matter, which is composed of nerve fibers.9 These children exhibited delays in cognitive function, language, and motor development.10 While evidence of such extreme neglect exists in the United States, most children in this country are at risk of suboptimal development from not enough positive stimulation or adverse childhood experiences.
Parental Stress and Parent-Child Interactions
As described above, parent-child interactions are critical in shaping brain development. Stress can be one of the most significant contributors to the impediment of parent-child interactions, with resultant long-lasting harm to the child’s brain development (Figure 1).
Figure 1 — Relationship Between Socioeconomic Status (SES), Stress, and Parenting on Language-Related Brain Physiology
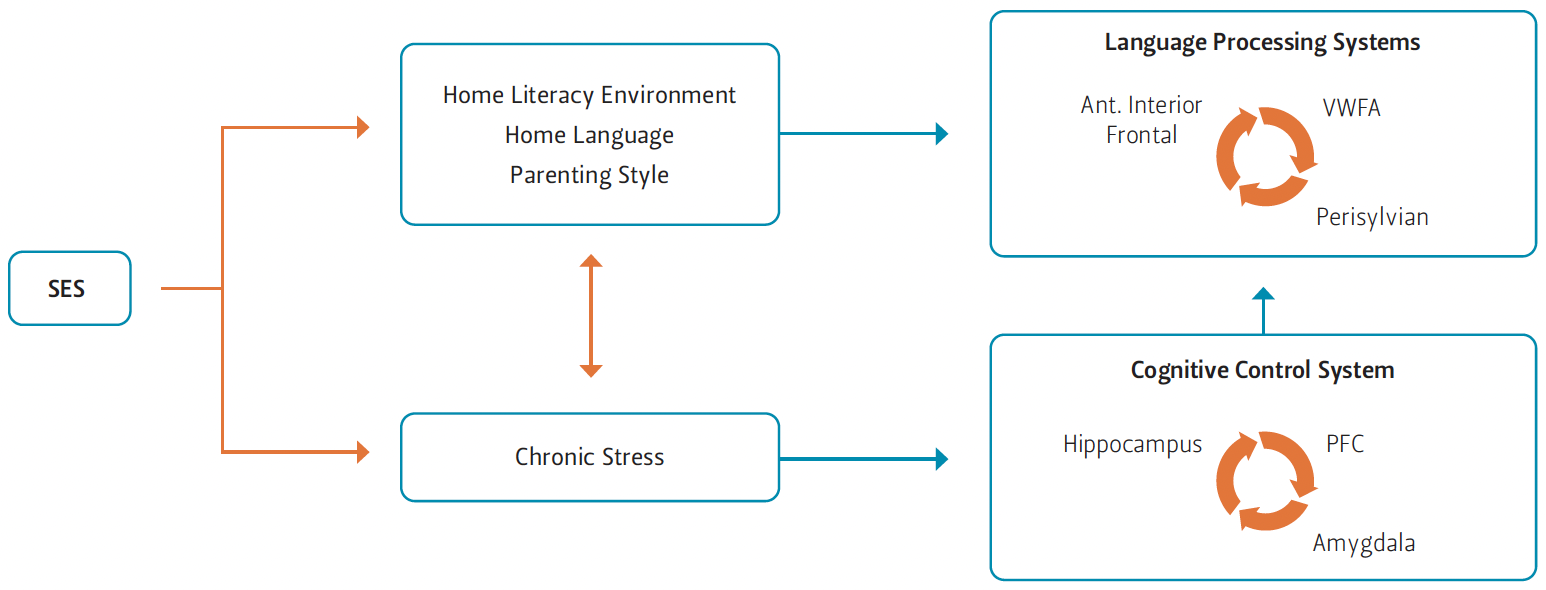
Note This figure depicts pathways linking low-socioeconomic status (SES) during childhood with language-related brain physiology via either parenting (upper) or chronic stress (lower). VWFA stands for Visual Word Form Area. PFC is prefrontal cortex.
Figure 1 depicts the negative impact that stress can have directly on the brain structures responsible for cognition, and indirectly on the brain structures responsible for language through parenting style and home environment.12 It is important to note that the alterations to the brain in the cited study persisted into adulthood.13 Also, the research supporting this depiction focused primarily on populations who live in poverty. Living in poverty restricts parental access to the resources, time, and built environment necessary to maximally support and stimulate their child’s growing brain. Limited resources also increase parental stress. For example, the “family stress model” connects economic distress, such as lack of institutional resources and exposure to economic hardships, to parental stress and resultant disruption of parent-child interactions.14 This model has been shown to explain the disparities in language, memory, and cognition between children in high income families and those in low-income families, and is supported by research demonstrating that economic hardship correlates strongly with parental stress and depression.15
The coronavirus pandemic is creating unprecedented financial, social, and external stressors that can hamper parent-child interactions. For instance, the pandemic has taken a toll on the U.S. economy, and many families are now either underemployed or unemployed. Approximately 36.5 million Americans have filed for unemployment benefits since shelter-in-place orders were enacted throughout the country in March 2020,16 and job losses will likely continue to mount as businesses struggle to remain open. This financial strain can severely impact parents’ mental and emotional health, particularly for families already living in poverty. In normal circumstances, job losses can have a devastating impact on families, but the additional strains of the pandemic may exceed parental coping abilities, thereby impacting parent-child interactions. In fact, research from other natural disasters indicates that we can expect parental stress and depression to rise during the current pandemic.17 Since parent-child interactions are critical to optimal brain development, the longer families are isolated and under severe strain, the greater the risk that children will not be getting the stimulation and responsive parenting that they need. The result will be long-term adverse effects on brain development, which will impact academic, economic, and health outcomes.
Prenatal Period
Just as excess cortisol in an infant or toddler may disrupt normal brain development, maternal cortisol may impact fetal brain development. While maternal stress has a more indirect impact on a child’s brain development, the impact of prenatal stress is more direct. Elevated stress hormones in the mother that persist during pregnancy deregulate an important protective placental enzyme that is responsible for converting maternal cortisol into an inactive form.18 High levels of maternal stress decrease the levels of this protective enzyme, thereby allowing cortisol to remain in its active form and cross the placenta.19 Fetal exposure to high levels of maternal cortisol are toxic to the developing brain and alter brain structures and neural connections that regulate cognition, emotions, and behavior in the child.20
An example of the long-term impact of prenatal maternal stress during a natural disaster can be found in the research conducted for “Project Ice Storm.” After an ice storm in the Canadian province of Quebec in January1998, a power outage lasting approximately 40 days affected more than 3 million residents.21 Millions were confined to their homes, unable to get to work or school. Incomes dropped and businesses closed, resulting in an estimated economic impact of $5.4 billion.22
Researchers began enrolling pregnant women in the project six months after the ice storm to investigate the long-term impact of disaster-related maternal stress on the developing child.23 Their sample primarily consisted of Caucasian, educated, middle-class women at various stages of pregnancy.24 Participants were asked to report their perceived stress levels (how stressed they felt during the storm) and objective disaster-related measures, such as injury and losses.25 The researchers evaluated the participants’ children at age 2 and again at age 5.5. They found that lower cognitive and language functioning correlated with objective measures of disaster stressors, but not with perceived stress, at age 2 and continued to persist at age 5.5.26 This finding suggests that objectively stressful external events during natural disasters have a greater impact on the developing child than the mother’s subjective reaction to those events. Moreover, since various brain structures are responsible for language (Figure 1), a decline in language functioning represents suboptimal development in multiple parts of the brain.
Lessons from Project Ice Storm are important because, compared to other natural disasters, the Covid-19 pandemic most closely resembles Quebec’s experience in terms of the economic impact, job losses, and social isolation resulting from being homebound. Moreover, it demonstrates that even those who are fairly well-positioned in society can experience negative effects from natural disaster stressors that have a long-lasting impact on their children. While lower income populations are at higher risk, natural disasters can produce physiological responses that can negatively impact the brain development of the next generation at any income level.
Parental Stress and Child Maltreatment
Under stressful circumstances, normally loving parents may uncharacteristically lash out at their child, physically or emotionally. Research demonstrates that parental stress can increase the likelihood of violence against children,27 and that parental stress and depression are correlated with an increase in child maltreatment.28 The normal internal regulation of parents is disrupted during times of profound stress, and they may find themselves striking or shunning their child.
While a clear relationship between sudden financial stress and child abuse has not been clearly demonstrated, there is data suggesting that for some populations, financial hardship can result in increased risk of child physical abuse. However, it is difficult to identify which populations are at risk because of limited data on the parental characteristics that increase the potential for child abuse. One study found that parental stress is a mediator between child behavior and child abuse potential.29 In other words, under stress parents perceive their child’s behavior in a more negative way, and that negative perception is associated with child abuse potential.30 Moreover, data from the 2018 U.S. financial crisis showed an increase in hospitalizations for infants with abusive head trauma in select hospitals.31 Additionally, recent research has demonstrated that the implementation of the earned income tax credit resulted in a decrease in hospitalizations for abusive head trauma in children.32
Unfortunately, it is difficult to ascertain whether child abuse cases rise during a natural disaster because the abuse may go unreported during the event. A counterintuitive outcome of the significant disruption caused by natural disasters (Hurricane Katrina, Hurricane Harvey, Covid-19) is a predictable decrease in reports of abuse to Houston’s Child Protective Services (CPS). Covid-19, for example, has isolated families and children from the social structures that provide support during times of hardship. For school-age children, teachers and counselors are often the first to recognize trouble at home, and are the most common reporters of maltreatment to CPS. With school closures, teachers can no longer act as community sentinels.
Children under the age of 5 are particularly vulnerable to child abuse,33 and inflicted brain injury can increase after natural disasters.34 As noted earlier, injuries to the brain are particularly damaging for young children, as the brain is rapidly developing and is most susceptible to injury during the first three years of life. Trauma and child abuse or neglect can irreversibly alter an already fragile brain architecture, causing life-long ramifications.
Opportunities for Intervention
Despite the significant disruption wreaked by the Covid-19 pandemic, there are opportunities to make meaningful inroads in addressing some of the structural and non-structural obstacles for families and communities. As there is uncertainty for what the “new normal” will be, now is the time to create new strategies that will strengthen and support families by mitigating the risk of natural disasters on families and bolstering resilience during times of stability.
First, in times of disruption, many families require attention to some of the important basics of survival. As framed in Maslow’s Hierarchy of Needs, “physiologic needs” require all energy of families living in unstable circumstances. These physiologic needs include air, water, food, shelter, sleep, and clothes.35 Given the major economic losses caused by the pandemic, it is important to have systems in place that allow agencies and nonprofits to identify and proactively reach out to families most at risk. Meeting families’ basic needs increases parental capacity to receive parenting support and to engage with their children in ways that reduce the risk of adverse brain development in their child. An example of such a system is food distribution by local school districts, some of which have opened distribution to all families, not just those with school-age children. However, it is unknown if all families in need have been able to access food distribution centers during times of crisis; a system that identifies and reaches out to families would be more likely to increase the scope and impact of such initiatives.
Second, as the growing brain is the most malleable in the first three years of life, there should be a new emphasis on early brain development. Cities and communities should foster a culture of prioritizing brain development during times of stability, and governmental and nonprofit organizations should be able to respond with tailored interventions that mitigate risks and support brain development during natural disasters. Moreover, access to high-quality childcare is critical: the return on investment of universal, evidence-based childcare is profound.36 City leaders should work with communities to identify neighborhoods with the largest educational gaps, and collaborate to develop the strategies and resources needed to ensure that all infants and young children have access to free or low-cost, high-quality childcare. Moreover, as seen in this pandemic, childcare centers have slim profit margins and are most at risk of closure when the economy contracts. State and local governments need strategies and resources to ensure that childcare centers can remain open in times of crisis.
Third, given the importance of health care and parental support in the parent-child relationship, communities should develop strategies that ensure access to pediatric health care. Health care delivery should also include an emphasis on parental support and responsive, nurturing parenting, integrated behavioral health for parents and all children, and a comprehensive strategy to address the social determinants of health of the family. This new health care delivery model could be financially feasible through innovative payment and reimbursement models that provide additional compensation for outcomes, not just fee for service. Additionally, practices that have strong community partnerships can ensure their patients receive additional services, and a shared cost-saving agreement between the clinic and community partner could help sustain the relationship.
Fourth, as social isolation can exacerbate pre-existing difficulties within families and create obstacles for those with young children to access resources, citywide initiatives should be developed to build virtual social networks and close the digital divide between resourced and under-sourced communities. In the event of a natural disaster, this network can be used to reach families and provide support to mitigate the risk of adverse parent-child interactions.
Policy Recommendations
Young children are a critical population that has been largely excluded from Covid-19 discussions and decision-making. Yet the impact of this pandemic on the next generation will be felt for many years to come. We have an opportunity now to create policies and practices that will mitigate parental stress and reduce the risk of suboptimal brain development in the next generation. While we do not want to be alarmist, the research presented in this brief is supported by decades of studies in many disciplines; all demonstrate the negative impact of parental stress, which is heightened during natural disasters, on brain development. The resultant cognitive and language delays will hinder academic ability and the potential for success in adulthood. We must plan now with the future generation in mind. Thus, we recommend the following policies.
Federal Government
1. Direct small business relief funds to childcare centers.
Congress has passed two stimulus packages that involve forgivable loans to small businesses. However, very small businesses are disproportionately denied these loans,37 and childcare centers, in particular, are vulnerable to closures due to very small profit margins. Childcare centers are important because they allow essential employees to go to work during the pandemic, and they provide access to stimulating, engaging environments for small children. Moreover, during this crisis, parents need a reprieve that allows them to engage in self-care and have time away from children if stress levels are high and there is a risk of child maltreatment.
2. Expand open enrollment of the Affordable Care Act and expand subsidies to help individuals purchase insurance.
Many workers have lost their jobs and as such have lost their health insurance. Lack of health insurance during a public health crisis is detrimental not only to families, but to our society as a whole. Although the federal government is covering Covid-19-related health care costs for the uninsured, many other important health care needs are going unmet, such as vaccinations, cancer screenings, and chronic health care follow-ups. Yet the federal government did not expand open enrollment for the ACA during the pandemic, leaving insurance options limited to state insurance exchanges.
3. Expand income tax credits.
As noted earlier, the data show that an expansion of the earned income tax credit for families has resulted in fewer hospitalizations for abusive injuries to children. In times of significant financial stress, a small amount of financial support will allow families to provide for the needs of their young children.
State/Local Governments
4. Increase parent support services.
As discussed, parent-child interactions are critical for supporting the brain development of young children. Yet social and economic factors can hinder these interactions and many parents are unaware of the long-term damage that adverse interactions can have on their child. Additionally, some parents did not have a model of appropriate parent-child interactions as a child and do not have access to such models now. Parenting classes can provide social support and ways to deal with stress while also teaching or strengthening parenting knowledge and skills. As seen in the Covid-19 pandemic, programs need to be flexible and able to rapidly adapt to virtual platforms. Ideally, if communities have established a culture of supporting brain development and strong social networks, existing relationships can be leveraged during a natural disaster to reach families in need. Overall, improved support for a parent’s ability to parent will result in improved outcomes for children.
5. Begin systematic data collection on families with young children.
Very little is known about the characteristics of families with small children or how many children are at risk for suboptimal brain development in Texas. Researchers make risk predictions based on race, income, and family demographics, but these are crude estimates that do not lend themselves to strategies for intervention and policy development. Additionally, research is needed to identify parental characteristics that put children at risk for maltreatment because as discussed above, aside from demographic predictors, the literature is sparse. Moreover, little is known about the impact of a pandemic on families and what kind of support would help foster resilience. Therefore, it is difficult to plan and implement effective policies and interventions that would bolster family well-being during stable economic and societal times, and include a disaster-readiness plan to mitigate potential harm to these families. Data-driven decision-making is critical to ensuring maximum impact of investments. Systematic data collection and research will optimize the opportunities to improve the brain development of the next generation and, it is hoped, reduce the inequities and societal costs that are associated with adverse brain development.
Endnotes
1. Quianta Moore, Claire Bocchini, and Jean Raphael, “Development of an evidence-based early childhood development strategy,” Rice University’s Baker Institute for Public Policy, September 2016, https://bit.ly/30XbOdG.
2. Ibid.
3. Ibid.
4. Sharon Fox, Pat Levitt, and Charles Nelson, “How the timing and quality of early experiences influence the development of brain architecture,” Child Development 81, no. 1 (Jan-Feb. 2010): 28-40.
5. Ibid.
6. SAMHSA, “Disaster Technical Assistance Center Supplemental Research Bulletin: Behavioral Health Conditions in children and youth exposed to natural disasters,” September 2018. Accessed on June 2, 2020, https://www.samhsa.gov/sites/default/files/srb-childrenyouth-8-22-18.pdf.
7. Sarah Miragoli, Stefania Balzarotti, Elena Camisasca, and Paola Di Blasio, “Parents’ perceptions of child behavior, parenting stress, and child abuse potential: individual and partner influences,” Child Abuse & Neglect 84 (2018): 146-156.
8. Jack P. Shonkoff, et al., “The lifelong effects of early childhood adversity and toxic stress,” Pediatrics 129, no. 1 (2012): e232-e246.
9. C.A. Nelson, N.A. Fox, and C.H. Zeanah, Romania’s Abandoned Children: Deprivation, Brain development, and the Struggle for Recovery (Cambridge, MA, and London, England: Harvard University Press, 2014).
10. Ibid.
11. Suzanne Perkins, Eric Finegood, and James Swain, “Poverty and language development: roles of parenting and stress,” Innovations in Clinical Neuroscience 10, no. 4 (2013): 10-19.
12. Ibid.
13. Ibid.
14. Laura Justice, Hui Jiang, Kelly Purtell, et al., “Conditions of poverty, parent-child interactions, and toddlers’ early language skills in low-income families,” Maternal and Child Health Journal 23 (2019): 971-978.
15. Ibid.; Perkins et al., “Poverty and language,” 2013.
16. Alan Berube, “What weekly unemployment claims reveal about the local impacts of the Covid-19 recession,” Brookings Institution, May 14, 2020, https://www.brookings.edu/blog/the-avenue/2020/05/13/what-weekly-unemployment-claims-reveal-about-the-local-impacts-of-the-covid-19-recession/.
17. Bihan Tang, Xu Liu, Yuan Liu, Chen Xue, and Lulu Zhang, “A meta-analysis of risk factors for depression in adults and children after natural disasters,” BMC Public Health 14, no. 1 (2014: 623.
18. Janiece DeSocio, “Epigenetics, maternal prenatal psychosocial stress, and infant mental health,” Archives of Psychiatric Nursing 32 (2018):901-906.
19. Mallory Bowers and Rachel Yehuda, “Intergenerational transmission of stress in humans,” Neuropsychopharmacology 41 (2016):232-244.
20. Jorg Bock, Kathy Rether, Nicole Groger, Lan Xie, and Katharina Braun, “Perinatal programming of emotional brain circuits: an integrative view from systems to molecules,” Frontiers in Neuroscience, February 5, 2014, https://doi.org/10.3389/fnins.2014.00011.
21. David Laplante, Alain Brunet, Norbert Schmitz, Antonio Ciampi, and Suzanne King, “Project Ice Storm: Prenatal Maternal Stress Affects Cognitive and Linguistic Functioning in 5 ½-year-old children,” Journal of the American Academy of Child Adolescent Psychiatry 47, no. 9 (2008):1063-1073.
22. Marilla Steuter-Martin and Loreen Pindera, “Looking back on the 1998 ice storm 20 years later,” CBC News, January 4, 2018. Accessed June 2, 2020, https://www.cbc.ca/news/canada/montreal/ice-storm-1998-1.4469977.
23. Laplante, “Project Ice Storm,” 2008.
24. Ibid.
25. Ibid.
26. Ibid.
27. Hamed Seddighi, Ibrahim Salmani, Mohhamad Javadi, and Saeideh Seddighi, “Child abuse in natural disasters and conflicts: a systematic review,” Trauma, Violence, and Abuse (2019), https://doi.org/10.1177/1524838019835973.
28. Heather Kennan, Stephen Marshall, Mary Alice Nocera, and Desmond Runyan, “Increased incidence of inflicted traumatic brain injury in children after natural disaster,” American Journal of Preventative Medicine 26, no. 3 (2004):189-193.
29. Miragoli, et al., “Parents’ perception of child behavior,” 2018.
30. Ibid.
31. J.N. Wood, et al., “Association of Pediatric Abusive Head Trauma Rates with Macroeconomic Indicators,” Academic Pediatrics 16, no. 3 (2016): 224-232.
32. J. Klevens, et al., “Effect of the Earned Income Tax Credit on Hospital Admissions for Pediatric Abusive Head Trauma, 1995-2013,” Public Health Reports 132, no. 4 (2017): 505-511.
33. Mary Overpeck, Ruth Brenner, Ann Trumble, Lara Trifiletti, and Heinz Berendes, “Risk factors for infant homicide in the United States,” New England Journal of Medicine 339 (1998):1211-1216.
34. Heather Kennan, et al., “Increased incidence of inflicted,” 2004.
35. A.H. Maslow, “A theory of human motivation,” Psychological Review 50, no. 4 (1943): 370–396.
36. J.J. Heckman, "Skill formation and the economics of investing in disadvantaged children," Science, June 30, 2006.
37. Perla Trevizo, “When small businesses can’t access PPP, local governments struggle to close gap,” Texas Tribune, June 5, 2020, https://www.texastribune.org/2020/06/05/texas-ppp-loans-small-businesses/.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


