
Introduction
In late 2019, the federal government finalized rules requiring hospitals to make public a list of their standard charges for the items and services they provide (Centers for Medicare & Medicaid Services 2020). This list must include the cash prices, as well as the minimum and maximum rates the hospital has negotiated with insurers. The Centers for Medicare & Medicaid Services (CMS) issued these rules, citing multiple studies concluding that a lack of price transparency is an important reason for rising health care costs. The announcement states, “We believe there is a direct connection between transparency in hospital standard charge information and having more affordable health care and lower health care coverage costs. We believe health care markets could work more efficiently and provide consumers with higher-value health care if we promote policies that encourage choice and competition.” Fewer than 20% of 100 randomly sampled hospitals were in full compliance with the new regulations in March 2021 (Gondi, Beckman, and Ofoje 2021). As of June 2021, 55% of the general acute care hospitals that treat Medicare patients had not met CMS requirements involving the reporting of commercial negotiated prices (Jiang et al. 2021).
This report examines Texas hospitals’ compliance with the CMS hospital price transparency regulations as of January 2022. Texas is of particular interest because its state legislature passed additional measures intended to increase hospitals’ financial penalty for noncompliance. The state comprises 8.9% of the U.S. population—the second-largest in the country—and has 9.4% of the nation’s hospitals (“Number of Hospitals in the U.S. by State as of 2020*” n.d.; United States Census Bureau 2021b).
Federal Legislation
Implemented through an executive order under the Trump administration and supported by the Biden administration, price transparency efforts have emerged as part of a bipartisan effort to reduce rising health care costs (CMS 2019). As of January 1, 2021, the federal government has required every hospital to provide a public list of standard charges for each of its locations that includes the following information for every service or good provided:
- Description of item/service (with an identification code including but not limited to a CPT, HCPCS, DRG, or NRC code)
- Gross charge
- De-identified minimum negotiated charge
- De-identified maximum negotiated charge
- Discounted cash price
- Any payer-specific charges (with the third party named)
The list must be provided in a single-file, machine-readable format named in the following manner: __ standardcharges.[json|xml|csv]. Each list must be displayed in a prominent location on the hospital’s website home page (or accessible through a designated web page clearly linked on the home page), be free to access, and not require any identifying information or an account registration.
All hospitals are also required to provide a list of shoppable services that includes all of the information outlined above in a consumer-friendly manner. Each list must include a minimum of 300 shoppable services (including as many of the 70 services identified as shoppable by the CMS that the hospital provides), with an exception for hospitals that provide fewer than 300 shoppable services and thus must furnish the necessary information for as many services as available. In place of a list, hospitals may also provide a price estimation tool that supplies the necessary information for the shoppable services offered, as long as the tool is free and does not require the user to create an account.
Hospitals not in compliance with the price transparency requirements are required to submit a corrective action plan for approval. Once the plan is approved, the hospital is required to immediately act on the corrective plan. CMS’ initial rules stated that failure to submit a corrective action plan or act in accordance with an approved plan could result in a maximum fine of $300 per day, totaling $109,500 yearly. The average net patient revenue for U.S. hospitals was estimated to be $334.5 million in 2018 (“Revenue Trends at U.S. Hospitals” n.d.), and hospital margins (payments minus costs, divided by payments) were 6.3% in 2020 (Binkowski et al. 2021). Therefore, many larger hospitals in the U.S. would find a $109,500 penalty to be inconsequential.
Recognizing the inadequacy of the penalty for nonreporting, CMS issued another final rule, effective January 2022, linking the size of the penalty to hospitals’ bed size. The updated rule assesses a penalty of $10 per bed per day for hospitals with a bed count greater than 30, not to exceed a maximum daily dollar amount of $5,500. Thus, the new maximum penalty amount for noncompliance by a hospital with 550 or more beds for an entire year is $2,007,500 (CMS 2021).
Texas State Legislation
To supplement the federal law, which came into effect on January 1, 2021, the Texas state legislature passed further measures to increase the penalty, as of September 1, 2021, on a graduated scale through S.B. 1137 (87th Texas Legislature 2021). The legislation includes a clause that states, “Each day a violation continues is considered a separate violation.” For example, by day three, a hospital that reported gross revenue exceeding $100 million in the preceding year would owe $1,000 for the first day of non-reporting, $2,000 for the second day, and $3,000 for the third day, totaling $6,000. Therefore, the daily penalty is meant to compound rapidly. Following the language of the legislation, the corresponding penalties for noncompliance are estimated in Table 1.
Table 1 — Estimated Fines for Texas Hospitals Not Posting Prices in Accordance With S.B. 1137

While S.B. 1137 took effect September 2021, the Texas Health and Human Services Commission did not issue guidance interpreting the law until February 3, 2022 (Texas Health and Human Services 2022). The commission’s guidance disregarded the clause in S.B. 1137 stating that each day of compliance should be considered a new violation. Therefore, a hospital with over $100 million in revenues during the previous year would be required to pay only $365,000 in fines instead of the $65 million intended by the state legislators who authored the bill.
Methods
We consulted the Texas Hospital Association (THA) website to construct a list of short-term acute care hospitals (Texas Hospital Association 2022). Behavioral health and long-term care hospitals were excluded from the list based on descriptive information in hospital names (e.g. “rehabilitative hospital”) and information posted on hospitals’ individual websites. We utilized each hospital’s website to locate its price transparency publications and evaluate it using three shoppable services: MRI Brain CPT 70553, Ultrasound Abdomen 76700, and Basic Metabolic Panel CPT 80048. We chose these three services because they are frequently used, they are prescribed for different patient populations, and nearly every general hospital offers them. We assumed that if the hospital followed the regulations for these three services, it likely complied with the bill.
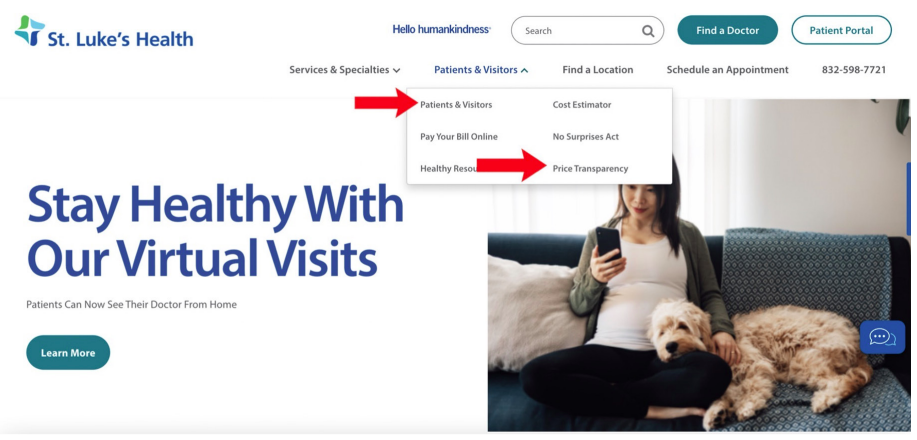
To find the machine-readable prices for each hospital, we started with the direct web page linked from the home page of its website. Typically, the subpage with the pricing transparency document resided either as a link on the top of the home page or existed as a subcategory on the page with information for patients and visitors. If the pricing information was unclear or difficult to find, we then searched the hospital name and “price transparency” or “standard charges” to find the necessary files. If a link to a designated machine-readable file did not yield the correct information or was an empty file, we assumed that the information was not published elsewhere on the website. Since the federal law permits a price estimator tool in place of a list of shoppable services, we exclusively checked the three services within the standard charges file, which does require all of the necessary information.
In Figure 1, we first located and clicked on the file. Then, we checked the file for the de-identified minimum and maximum negotiated charges, the cash prices, and the gross prices for the three shoppable services.
Figure 1 — Example of Where to Find Machine-Readable Price Data on a Hospital Home Page
We aimed to gain a sense of whether the federal and Texas penalties for noncompliance pose a significant financial burden on the state’s largest health care systems. For five large systems, we estimated the federal penalty that would be levied for noncompliance for an entire year using their reported hospital bed count in 2019. We then compared the magnitude of these fines to the hospitals’ operating profits as reported in their 2019 Medicare cost reports using a methodology developed by the National Academy for State Health Policy (National Academy for State Health Policy 2021).
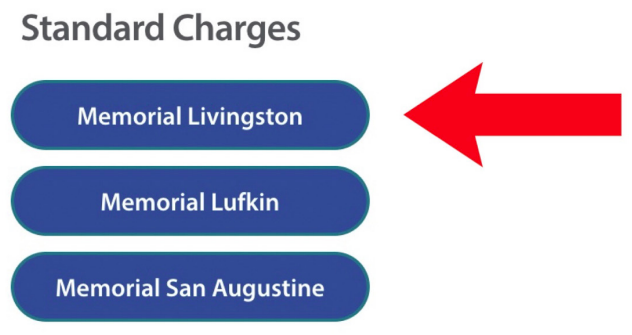
Figure 2 — Example of Subpage That Links to Price Data For Individual Hospitals That Belong to a Health Care System
Results
The link below provides a list of Texas short-term acute care hospitals and their compliance with the CMS requirements to post the different types of prices for shoppable services (yes/no) and provide price data in a machine-readable format (yes/no):
https://rice.box.com/v/ DataTXHospPriceTransparency
If any of the information was not present, the hospital was marked “No” under the shoppable services column. The second column, “Machine-readable,” is only noteworthy for the hospitals that published their standard charges but did not do so in a machine-readable format, resulting in a different search-interface that makes data discovery difficult and violates the federal law. In these instances, the “Shoppable Service” column was marked “Yes” and the “Machine-readable” column was marked “No.” If the hospital did not publish sufficient information on standard charges, but did post the information in a machine-readable file, the “Machine-readable” column was marked “N/A.”
Figure 3 — Example of Price Data in a Machine-Readable File for a Hospital
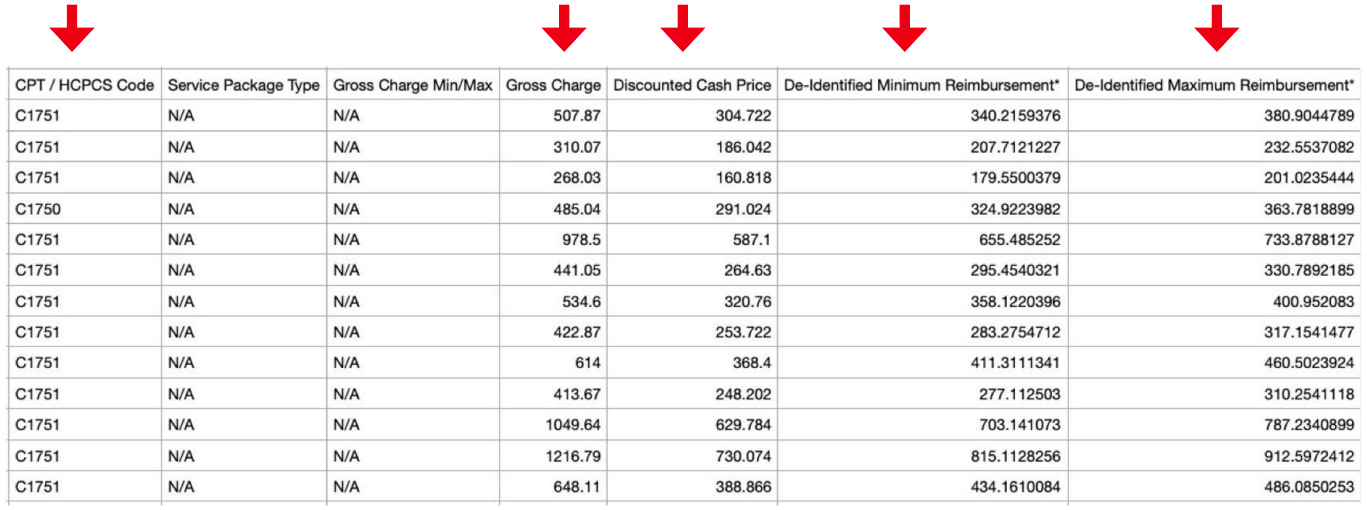
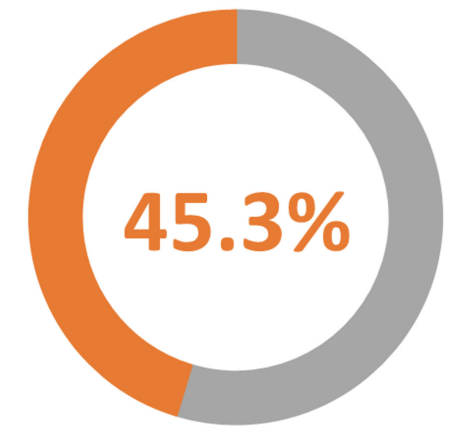
Figure 4 — Percentage of Texas Hospitals Complying With CMS Price Transparency Rules
While verifying compliance for each hospital, we found that hospitals that made their price transparency documents harder to find were more likely to be noncompliant (i.e., only reporting the cash prices and not the de-identified minimum or maximum negotiated prices with insurers). Many of the hospitals in full compliance had links to their prices that were plain and easy to find on their home pages. At some hospital websites, the link to a price transparency document did not work and simply reloaded the page.
In total, the Texas hospital price compliance rate is 45.3%, meaning that less than half of the hospitals are complying.
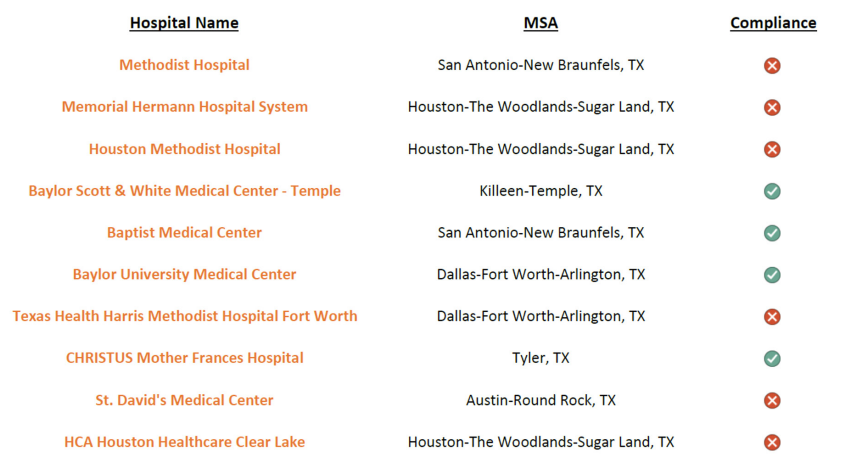
Using the list at https://dexur.com/usa/ state-tx/, we identified price transparency compliance among the top 10 hospitals in Texas, ranked by their annual number of Medicare inpatient discharges. Only 40% of Texas’ largest hospitals were in compliance.
Figure 5 — Compliance With CMS Price Transparency Rules Amongst Texas’ 10 Largest Hospitals
In Figure 6, we calculated the percentage of complying hospitals by metropolitan statistical area (MSA). We selected the six largest MSAs in Texas, which comprise 72.9% of the state’s population (United States Census Bureau 2021a). Hospitals in the remaining cities were counted in the category “other areas.” We assigned hospitals to MSAs by matching the county reported on the THA website to the Quarterly Census of Employment and Wages County-MSA pairing reported by the U.S. Bureau of Labor Statistics (U.S. Bureau of Labor Statistics n.d.). For hospitals missing county information on the THA website, the city listed on the THA website was matched to the corresponding county using Simplemaps’ United States Cities Database prior to MSA assignment (Simplemaps 2021).
Figure 6 — Percentage of Hospitals Complying With CMS Price Transparency Rules by Metropolitan Statistical Area
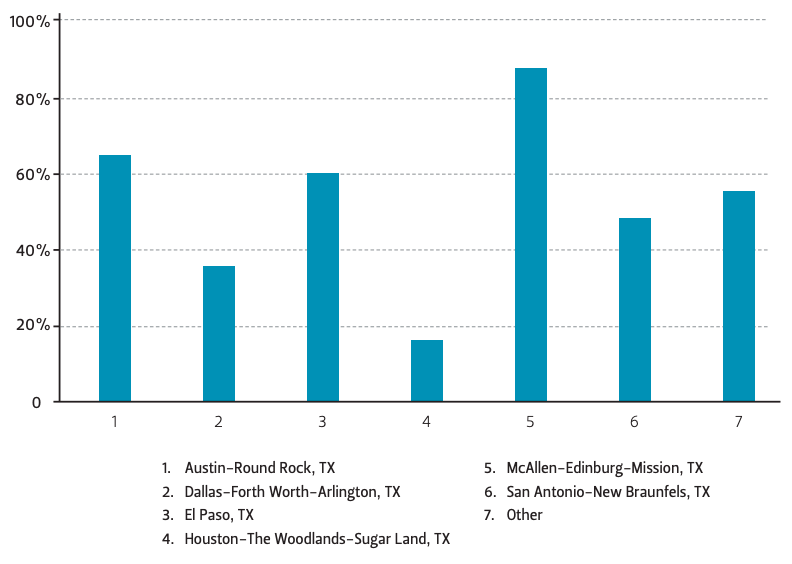
Based on our calculations, the McAllen-Edinburg-Mission MSA had the highest rate of compliance (88%), while the HoustonThe Woodlands-Sugar Land MSA had the lowest compliance rate (16%). However, the high compliance rate in the McAllen MSA may be attributed to the relatively low number of hospitals in that area. The Houston MSA’s relatively low compliance percentage is heavily influenced by three large health care systems that have skirted the price transparency requirements. These noncompliant systems each have multiple facilities that did not post their prices. Out of the larger, well-known cities, the San Antonio-New Braunfels and AustinRound Rock MSAs performed relatively better than the Houston and Dallas MSAs, with compliance rates of 48% and 65%, respectively. We observed that smaller hospitals in rural areas were more likely to comply than larger hospitals, which is why the compliance rate for “Other” is relatively high.
We examined five large health care systems in Texas and found that two were posting their prices, while three were not (see Table 2). The estimated fine for noncompliance for an entire year relative to profits is relatively high for Baylor Scott & White Health (9.8%), which does post its prices. Christus Health had also posted its prices as of January 2021, despite initial resistance as reported by the Wall Street Journal (Evans, Mathews, and McGinty 2021). This system posted negative profits, so a fine would have caused additional damage to its financial standing. In contrast, Houston Methodist and Memorial Hermann do not post their prices, and the federal fines appear small relative to their profits in 2019 (1.3% and 2.7% respectively). The fine as a share of profits for Catholic Health Initiatives (-10.4%) suggests that this system should feel compelled to comply with the regulations, but it has not done so yet.
Table 2 — Estimated Fine for Select Health Care systems Based on Hospital Bed Count and Operating Profits in 2019 for Noncompliance with CMS Price Transparency Regulations*

Note *Estimated fine for not reporting for 365 days.
Conclusion
When CMS issued its price transparency rules, it cited multiple studies supporting the benefits of requiring hospitals to report more comprehensive price information (Scheurer 2013; Bees 2019; Wetzell 2014; Robert Wood Johnson Foundation 2016; Boynton and Robinson 2015). Increasing numbers of insurees have high-deductible health insurance plans and are eager to choose lower-cost providers, because the consumer must cover 100% of costs outof-pocket below the deductible. Improved transparency can also directly benefit employers, who need this information to make informed choices between health plans, providers, and treatments. For example, employers need price transparency in order to implement reference-pricing strategies that encourage their insured workers to use high-volume, lower-cost hospitals and surgeons that provide good treatment outcomes.
As our research shows, as of January 2022, only 45% of Texas hospitals were compliant with federal and state price transparency legislation. This compliance rate is equal to the rate reported for all U.S. hospitals back in June 2021 (Jiang et al. 2021). A December 2021 Wall Street Journal article reported that CMS had issued 335 warnings to hospitals for violations of the price transparency rules, but no fines have been issued yet (Evans, Mathews, and McGinty 2021). The article mentioned that early in 2021, Texas-based Christus Health said on its website that it did not plan to comply with the rules, because its comprehensive list of prices would “only be useful for [its] competitors.” Five Christus hospitals received warning letters from CMS, and we determined that all Christus hospitals are now posting their prices. Even so, our estimates of the size of the federal fines relative to annual profits for two of Texas’ largest health care systems are relatively small. For these systems, only the magnitude of the fines approved by the state legislature—the only penalty mechanism discussed by the CMS—would be sufficient to achieve compliance.
U.S. health care costs have risen faster than gross domestic product for decades, and they will continue to do so after the pandemic ends. Rising hospital prices are one of the major reasons underlying this cost growth (Cooper et al. 2019). Research has documented the link between hospital mergers and acquisitions and higher prices (Dafny 2018), and suggests that large health care systems are a prime contributor to cost growth. Texas state legislators were correct to craft legislation that would impose extraordinary penalties on the largest health care systems for failing to make their prices transparent to consumers, employers, and policymakers. Until S.B. 1137 is implemented as intended, Texans will lack the tools they need to shop for reasonably priced, effective hospital care.
References
87th Texas Legislature. 2021. “S.B. No. 1137.” S.B. 1137. September 1, 2021. https://capitol.texas.gov/tlodocs/87R/billtext/pdf/SB01137F.pdf#navpanes=0
Bees, Jon. 2019. “Is Transparency the Answer to Rising Health Care Costs?” New England Journal of Medicine Catalyst, March. https://catalyst.nejm.org/doi/full/10.1056/CAT.19.0686.
Binkowski, Alison, Jeff Stensland, Dan Zabinski, Ledia Tabor, and Brian O’Donnell. 2021. “Assessing Payment Adequacy and Updating Payments: Hospital Inpatient and Outpatient Services; and Mandated Report on Bipartisan Budget Act of 2018 Changes to the Low-Volume Hospital Payment Adjustment.” MedPAC, December. https://www.medpac.gov/wp-content/uploads/2021/09/Hospital-update-MedPAC-Dec-2021.pdf.
Boynton, Ann, and James C Robinson. 2015. “Appropriate Use of Reference Pricing Can Increase Value.” Health Affairs, July. https://www.healthaffairs.org/do/10.1377/forefront.20150707.049155/full/.
Centers for Medicare & Medicaid Services. 2019. “Medicare and Medicaid Programs: CY 2020 Hospital Outpatient PPS Policy Changes and Payment Rates and Ambulatory Surgical Center Payment System Policy Changes and Payment Rates. Price Transparency Requirements for Hospitals To Make Standard Charges Public.” A Rule by the Health and Human Services Department. November 27, 2019. https://www.federalregister.gov/documents/2019/11/27/2019-24931/medicare-and-medicaid-programs-cy-2020-hospital-outpatient-pps-policy-changes-and-payment-rates-and.
———. 2020. “Medicare and Medicaid Programs: CY 2020 Hospital Outpatient PPS Policy Changes and Payment Rates and Ambulatory Surgical Center Payment System Policy Changes and Payment Rates. Price Transparency Requirements for Hospitals to Make Standard Charges Public.” http://www.regulations.gov/.
———. 2021. “CMS OPPS/ASC Final Rule Increases Price Transparency, Patient Safety and Access to Quality Care.” November 2, 2021. https://www.cms.gov/newsroom/press-releases/cms-oppsasc-final-rule-increases-price-transparency-patient-safety-and-access-quality-care .
Cooper, Zack, Stuart Craig, Martin Gaynor, Nir J. Harish, Harlan M. Krumholz, and John van Reenen. 2019. “Hospital Prices Grew Substantially Faster Than Physician Prices For Hospital-Based Care In 2007–14.” Health Affairs 38 (2): 184–89. https://doi.org/10.1377/hlthaff.2018.05424.
Dafny, Leemore. 2018. “Health Care Industry Consolidation: What Is Happening, Why It Matters, and What Public Agencies Might Want to Do About It.” In Testimony Before the House Committee on Energy and Commerce Subcommittee on Oversight and Investigations.
Evans, Melanie, Anna Wilde Mathews, and Tom McGinty. 2021. “Hospitals Still Not Fully Complying with Federal Price-Disclosure Rules.” Wall Street Journal, December 30, 2021. https://www.wsj.com/articles/hospital-price-public-biden-11640882507.
Gondi, Suhas, Adam L. Beckman, and Avery A. Ofoje. 2021. “Early Hospital Compliance With Federal Requirements for Price Transparency.” JAMA Intern Med 181 (10): 1396–97. https://doi.org/10.1001/jamainternmed.2021.2531.
Jiang, John Xuefeng, Daniel Polsky, Jeff Littlejohn, Yuchen Wang, Hossein Zare, and Ge Bai. 2021. “Factors Associated with Compliance to the Hospital Price Transparency Final Rule: A National Landscape Study.” Journal of General Internal Medicine. https://doi.org/10.1007/s11606-021-07237-y.
National Academy for State Health Policy. 2021. “How to Complete NASHP’s Hospital Cost Tool.” November 7, 2021. https://www.nashp.org/how-to-complete-nashps-hospital-cost-tool/.
“Number of Hospitals in the U.S. by State as of 2020*.” n.d. Statista. Accessed February 14, 2022. https://www.statista.com/statistics/710528/hospital-number-in-us-by-state/.
“Revenue Trends at U.S. Hospitals.” n.d. Definitive Health care. Accessed February 14, 2022. https://www.definitivehc.com/blog/revenue-trends-at-u.s.-hospitals.
Robert Wood Johnson Foundation. 2016. “How Price Transparency Can Control the Cost of Health Care.” https://www.rwjf.org/en/library/research/2016/03/how-price-transparency-controls-health-care-cost.html.
Scheurer, Danielle. 2013. “Lack of Transparency Plagues U.S. Health care System.” The Hospitalist. May 1, 2013. https://www.the-hospitalist.org/hospitalist/article/125866/health-policy/lack-transparency-plagues-us-health-care-system.
Simplemaps. 2021. “United States Cities Database.” August 13, 2021. https://simplemaps.com/data/us-cities.
Texas Health and Human Services. 2022. “Health Facility Compliance Guidance Letter.” February 3, 2022. https://www.hhs.texas.gov/sites/default/files/documents/gl-21-2008.pdf.
Texas Hospital Association. 2022. “Public List of Texas Hospitals.” 2022. https://store.tha.org/PersonifyEbusiness/Services/Consumer-Information/Public-List-of-Texas-Hospitals.
United States Census Bureau. 2021a. “Metropolitan and Micropolitan Statistical Areas Population Totals and Components of Change: 2010-2019.” October 8, 2021. https://www.census.gov/data/tables/time-series/demo/popest/2010s-total-metro-and-micro-statistical-areas. html.
———. 2021b. “State Population Totals and Components of Change: 2020-2021.” December 20, 2021. https://www.census.gov/data/datasets/time-series/demo/popest/2020s-state-total.html#par_textimage_500989927
U.S. Bureau of Labor Statistics. n.d. “QCEW County-MSA-CSA Crosswalk.” Quarterly Census of Employment and Wages. Accessed February 14, 2022. https://www.bls.gov/cew/classifications/areas/county-msa-csa-crosswalk.htm.
Wetzell, Steve. 2014. “Transparency: A Needed Step Towards Health Care Affordability.” American Health Policy Institute. https://www.americanhealthpolicy.org/Content/documents/resources/Transparency%20Study%201%20-%20The%20Need%20for%20Health%20Care%20Transparency.pdf.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


