
Abstract
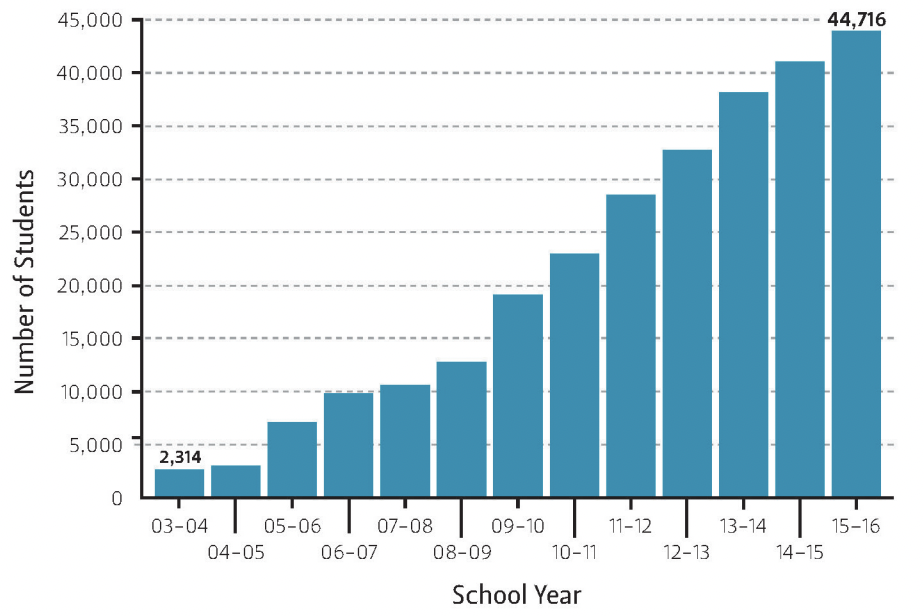
Vaccination is a robust intervention to prevent infectious diseases on an individual and community level. However, vaccination rates are below recommended levels throughout the world, including in developed countries. According to the National Immunization Survey, only 71.6 percent of children aged 19-35 months in the United States received the recommended combined series of vaccinations in 2014, and 0.8 percent of children were not vaccinated at all (Centers for Disease Control and Prevention 2015). Inadequate coverage is largely due to the increasing number of parents who opt their children out of vaccinations required for school entry. In Texas, approximately 45,000 nonmedical exemptions were filed across all age groups during the 2015–16 school year, a record high in the last decade and a figure that is only increasing. Parents who abstain from getting their children vaccinated often have misguided concerns regarding vaccine safety and utility. Recent outbreaks of vaccine-preventable illnesses, including large measles outbreaks in Texas, reflect the decreasing strength of herd immunity and result in billions of dollars in annual medical expenditures as well as indirect costs accounting for work loss and declines in economic productivity (McLaughlin et al. 2015). As one of the states with the least restrictive vaccine exemption laws in the country, Texas should make obtaining nonmedical exemptions more rigorous in order to avoid the public health risks and costs associated with preventable diseases.
Vaccines: Individual and Public Good
The goal of vaccines is to prevent serious diseases. Vaccines work by mimicking the disease-causing agent—a virus or bacteria—in order to strengthen the host’s immune defenses. Similar to medications, all vaccines and any additional components added to the vaccine to improve effectiveness, such as adjuvants (strengtheners), preservatives, and stabilizers, undergo rigorous testing by the U.S. Food and Drug Administration (FDA) for safety and efficacy (CDC 2013). Clinical studies also have tested vaccines in groups to optimize synergistic effects and determine appropriate vaccination schedules. In the United States, the Advisory Committee on Immunization Practices (ACIP) recommends distinct vaccine regimens for infants, adolescents, and adults.
Figure 1 — Decline in Immunization Coverage of Texas Kindergarteners
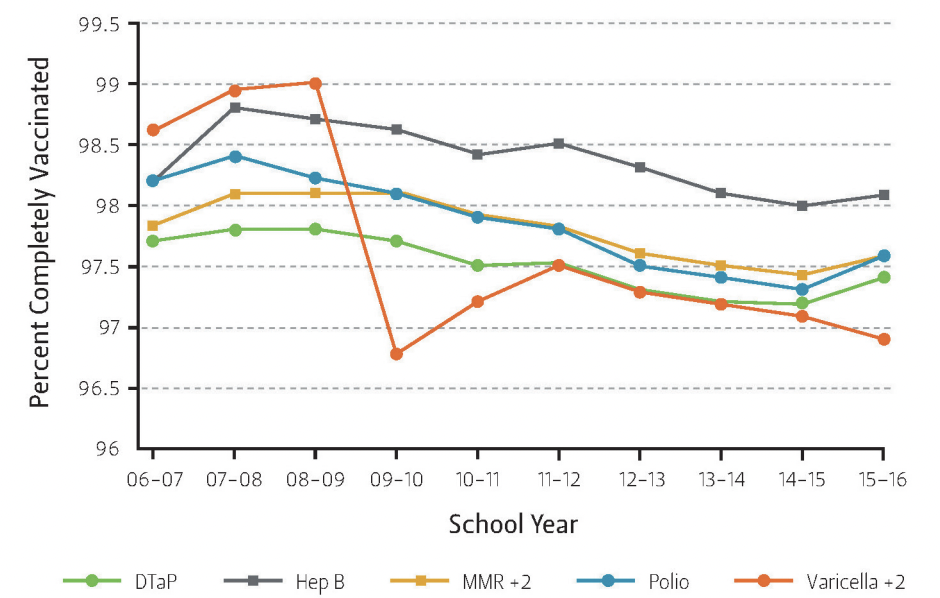
Vaccinations not only benefit an individual’s health but also that of the greater population. This includes people who cannot get vaccinated for medical reasons, chemotherapy patients, and immune-compromised individuals, as well as patients more susceptible to disease, including infants and the elderly. The strength of a population’s resistance to disease, also referred to as herd immunity, is directly related to the number of individuals who are immune. When most of the population is immunized, disease can be contained to minimize outbreaks (Fefferman and Naumova 2015). The U.S. Department of Health and Human Services (DHHS) identifies 90 to 95 percent as the target population coverage for most vaccine-preventable diseases; this range serves as the threshold needed to achieve the desired herd immunity effect (U.S. Department of Health and Human Services 2016). Vaccination rates that fall short of the population immunity threshold can selectively introduce increased disease incidence in older populations and more severe illness in all affected individuals, a mechanism known as the herd severity effect. Ironically, the risk of death from measles has increased significantly from 11 to 85 per 100,000 since the pre-vaccination era because children are not vaccinated during adolescence, resulting in more virulent infection later in life (Fefferman and Naumova 2015). Low willingness to vaccinate, and the health risks it poses to the general public, requires immediate attention from public health strategists and state-level policymakers.
Furthermore, vaccination is a good economical investment. Among children born in the United States from 1993 to 2013, it is estimated that vaccination will prevent 322 million illnesses and save $1.38 trillion in total societal costs (Whitney et al. 2014). For every $1 spent on the diphtheria, tetanus, and pertussis (DTaP) vaccine, $27 is saved. Similarly, every $1 spent on the measles, mumps, and rubella (MMR) vaccine saves $23, while the vaccine for varicella (chickenpox) saves $5.40 (Smith 2003). Responding to disease outbreaks also costs the state public health department significant time and money. The financial burden of an epidemic includes investigation, containment, medical care, and family expenses. For instance, the California Department of Public Health spent between $1.56 million and $3.91 million, excluding costs to health care facilities, to respond to the Disneyland measles outbreak in 2014-15 that affected 131 individuals (Harriman 2015).
Vaccine Hesitancy and Nonmedical Exemptions
In recent years, hesitancy toward vaccines has contributed to decreasing coverage rates in the developed world. Severe side effects of vaccination are rare—occurring in 1 per million cases—although there have been reported cases of allergic reactions and seizures. Low vaccination rates fall into two distinct population categories: under-vaccinated children, who are more often black and come from households near the federal poverty level with low educational attainment; and unvaccinated children, most often non-Hispanic white children, who on average come from households that are wealthier, educated, and covered by private health insurance (Smith et al. 2011).
In the past, vaccines were erroneously linked to specific medical conditions; the most common misconception is a purported link between the MMR vaccine and autism, a claim that has since been proven false. Disgraced medical researcher Andrew Wakefield falsified evidence linking the MMR vaccine to autism in a paper published in The Lancet in 1998, causing a surge in parents opting their children out of vaccinations. Additionally, several celebrities propagate this pseudoscientific claim, undermining confidence in vaccination despite scientific consensus of its safety and efficacy. The internet and popular media also help perpetuate the negative perception of vaccines through anecdotal stories of adverse events on non-credible websites.
Parents concerned about perceived risks of vaccinations may obtain exemptions for school mandated vaccines, a process that is regulated at the state level. Each state’s regiment is determined by the state’s health department but generally complies with ACIP recommendations. Generally, opt-out permission can be granted on the basis of medical necessity, religious faith, and philosophical beliefs. Nonmedical exemptions represent a conscientious decision not to vaccinate and generally encompass religious and philosophical exemptions. Before 2015, Mississippi and West Virginia were the only two states that banned religious and philosophical belief exemptions, although several bills that would allow such exemption claims were introduced in the 2016 legislative sessions. More recently, California banned nonmedical exemptions following the measles outbreak at Disneyland.
Infection risk has been linked to nonmedical exemptions to vaccination. Sixty-seven percent of vaccine-eligible patients who contracted measles during the 2014–15 Disneyland outbreak intentionally opted out of vaccination due to personal beliefs (Zipprich 2015). Those who opt out of vaccinations for religious or personal reasons are 35 times more likely to contract measles than their vaccinated counterparts (Diekema 2014). Furthermore, the tendency for vaccine-refusing populations to cluster geographically increases the risk for public outbreaks. In contrast, Mississippi, which banned nonmedical exemptions, has led the nation in pediatric vaccination rates since 1999 with more than 99 percent coverage of kindergarteners for the MMR, DTaP, and chickenpox vaccines (Seither et al. 2015). Notably, the Mississippi State Department of Health has not reported a single measles case in the state since 1992 (Mississippi State Department of Health 2008).
Vaccination Rates and Exemptions in Texas
Texas, similar to other states, has seen declining immunization rates over the past decade (Figure 1). High costs, constrained access, and inadequate health insurance coverage prevent proper and timely vaccinations. As a result, crowded urban areas, particularly around Houston and Dallas, and poor, rural areas, including counties along the U.S.-Mexico border, are affected by high levels of vaccine-preventable diseases.
Figure 2 — Increasing Number of Texas Students of All Grades Obtaining Conscientious Exemptions
Since 2003, Texas has permitted exemption from immunization for religious and personal beliefs. To obtain an exemption, a parent or legal guardian must file an affidavit, which is valid for two years, with the school. Additionally, there must be signed acknowledgment of having read the supplemental information, “The Benefits and Risks of Vaccination.” In a state of emergency or during an epidemic, students with conscientious exemptions may be excluded from attending school. Nonmedical exemption rates differ considerably throughout the United States. Texas’ nonmedical exemption rate, at 1.3 percent, falls just below the national median of 1.5 percent (Seither et al. 2015).
Figure 3 — Map of Texas Counties With Highest and Lowest Percentages of Students of All Grades Filing for Conscientious Exemptions, 2015–16 School Year
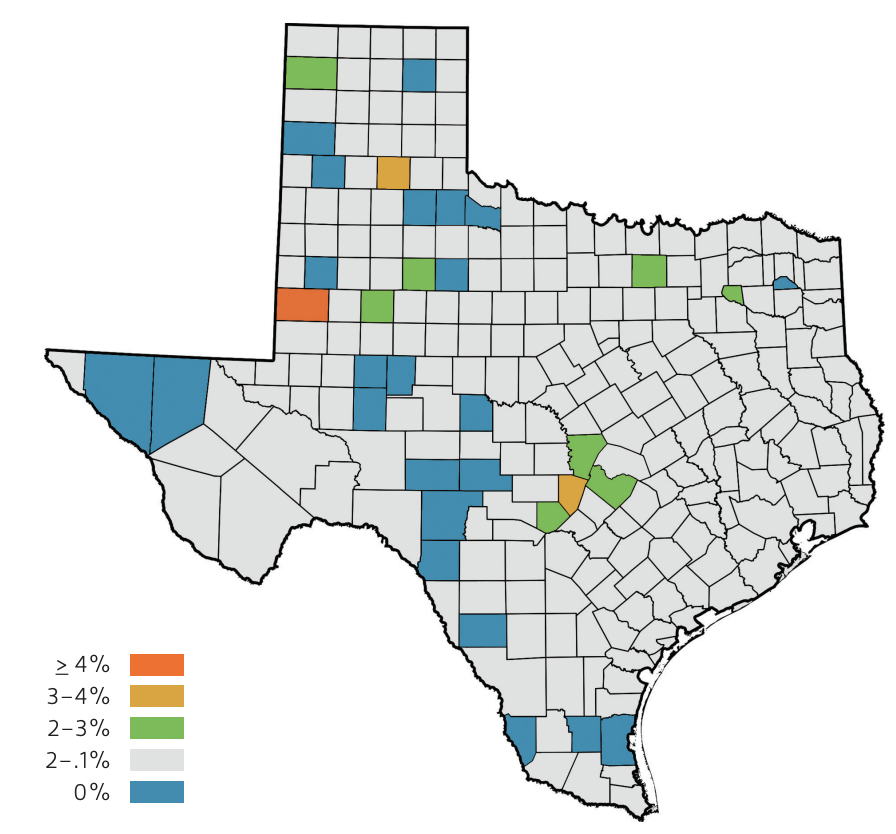
Although the overall exemption rate in Texas appears low, the number of conscientious exemptions has risen appreciably over the past decade (Figure 2). These exemptions are disproportionally utilized throughout the state, with one geographic cluster located in and around the city of Austin (Figure 3). In the 2015–16 school year, 2.30 percent of Travis County students obtained exemptions, which likely contributed to surges in vaccine-preventable diseases in the area (Texas Department of State Health Services 2016). Exempting communities in central Texas are comprised of residents who are primarily Caucasian, earn high incomes, and reside in suburban communities.
In contrast, several counties with roughly zero conscientious exemptions filed in the 2015–16 school year were less wealthy and located on the U.S.-Mexico border. In general, children in Central America have higher vaccination rates than children who reside in Texas. In 2014, 97 percent of children in Mexico received measles and rubella vaccinations while only 91 percent of children in the United States did (World Health Organization and UNICEF 2016). Low conscientious exemption rates near the U.S.-Mexico border reflect the willingness of Hispanic immigrants to vaccinate their children. However, many children in these communities tend to be under-vaccinated due to lack of access and high costs, which are common influences of health disparities associated with recent immigrants.
Even in counties with low vaccination exemption rates, there are pockets of individual schools with very high exemption rates that are often, but not always, linked to religious communities. Harris County had a low average exemption rate of 0.62 percent, yet some private, religiously affiliated schools reported substantial exemption rates, including Covenant Academy, a nondenominational Protestant Christian K-12 school where 8.45 percent of students opted out of vaccinations (TDSHS 2016). In 2013, a measles epidemic originated at Eagle Mountain International, an Evangelical Christian church near Dallas in Tarrant County. Although more than 98 percent of kids county-wide were vaccinated, more than 10 percent of the small congregation opted out of vaccinations, which left the community at risk. Even though most major religions do not oppose vaccination, tight-knit religious communities with higher levels of unvaccinated kids are hot spots for vaccine-preventable diseases (Grabenstein 2013).
As a result of the Disneyland outbreak, seven bills aiming to make vaccination exemptions on the basis of conscience more difficult to obtain were proposed during the 2015 Texas legislative session. None of them passed. These bills have generally not gained traction, as legislators instead favor promoting educational initiatives about vaccine safety over limiting individual rights to opt out (Rosenthal 2015).
Policy Recommendations
To reverse the trend of increasing vaccine exemptions in Texas, public health considerations should override personal autonomy. The Texas Legislature should employ a multifaceted approach to address school-entry vaccine exemptions. In a recent study, Texas was ranked as one of the least effective states in addressing vaccine-preventable diseases (Bradford and Mandich 2015). The study assessed vaccination exemption policies, including nonmedical exemptions, physician signature requirements, and punishment for noncompliance, and factored in county-level health and population characteristics as well as statewide economic conditions. Notably, Texas and other states that were characterized as less effective in managing the rise in vaccine-preventable diseases had higher statewide pertussis incidences. Since immunization policies are decided at the state level, policymakers must account for the racial, socioeconomic, and religious diversity throughout the state while remaining sensitive to popular political positions. For instance, California’s strong stance on vaccination may not be the right approach in Texas, particularly as Governor Greg Abbott has spoken against the “Californication” of state policies.
In order to increase coverage among school children, Texas policymakers should either ban conscientious exemptions or make the process of obtaining an exemption stricter by requiring a pediatrician’s signature and mandating that exemption claims be submitted annually. In 2014, Oregon passed a law requiring parents to submit a physician's signature or certificate of completion of an online educational module about the benefits and risks of vaccination. In the 2014-15 school year, there was a 17 percent decline in kindergarteners with nonmedical exemptions in the state, indicating greater informed choice and herd immunity (Oregon Health Authority 2015). In addition, the state could apply pressure on or offer incentives to private school boards to encourage full participation in vaccination programs. Private schools also could require parents to consult their family physicians before permitting their children to matriculate. This method fosters discussion with knowledgeable health care providers and increases the probability of vaccine uptake.
Other policies should be implemented to help understand the scope of the problem, including requiring schools and the state health department to publish the number of students on each campus who are vaccinated, under-vaccinated, and unvaccinated in a uniform and transparent system. Increased transparency will help eliminate gaps in current vaccination data and inform parents of local vaccination rates, which could potentially impact their decisions on which schools their children will attend. State action that addresses exemptions, while remaining sensitive to preserving parents’ abilities to make decisions surrounding their children’s health, is necessary to increase immunization rates in an era that has already experienced several outbreaks of vaccine-preventable diseases.
Vaccines are one of most cost-effective public health measures. Therefore, the state should encourage options for individuals who cannot afford vaccines. One of the best state programs is Texas Vaccines for Children (TVFC). More than 6,500 TVFC providers administer free vaccines to uninsured or underinsured children, children covered by the state Children’s Health Insurance Program (SCHIP), and children of Native American or Native Alaskan heritage. Additionally, more than 3.5 million Texas children on Medicaid can be vaccinated for free. The state could also provide incentives to increase provider enrollment in TVFC, particularly in regions with minimal coverage, and publicly acknowledge participating health clinics.
Medical schools within the state should work to improve physician communication related to health care and health literacy, such as strategies on interacting with patients when discussing controversial medical interventions, including vaccines. This communication method serves to emphasize the routineness of vaccination and minimize opportunities for parents to reconsider vaccinating their children (Opel et al. 2013). In a survey on resources for vaccine-related information, the majority of parents cite physicians as their most trusted source (Opel et al. 2013). Thus, it is vital that providers consistently and effectively reassure parents of the safety and efficacy of vaccines.
Furthermore, Texas should collaborate with both local health organizations and influential celebrities to distribute evidence-based, physician-approved educational materials and other resources in schools, community health clinics, pharmacies, supermarkets, and additional locations that dispense medications and administer vaccinations. Religious centers may be a great asset in disseminating information to Hispanic immigrants and other low-income populations (Grabenstein 2013). Additionally, distribution of materials in schools may be particularly useful to educate immigrant populations who typically do not know of or utilize the health resources available in schools. Offering vaccinations and informational brochures in multiple languages in school health offices and through social advocacy networks may remove the access barriers to vaccines and help increase willingness to vaccinate.
Too often, state policymakers fail to amend voluntary vaccination opt-out procedures to improve coverage rates and prevent disease outbreaks. Vaccine refusal undermines population-level benefits and epidemic preparedness of herd immunity. The state of Texas should work to maximize public health benefits and reduce health care costs through reforming policies on school-entry vaccine exemptions.
Endnotes
Bradford, W. David and Anne Mandich. 2015. “Some State Vaccination Laws Contribute To Greater Exemption Rates And Disease Outbreaks In The United States.” Health Affairs 34(8): 1383-90.
Centers for Disease Control and Prevention (CDC). 2013. “Understanding How Vaccines Work.” Accessed September 1, 2015. http://www.cdc.gov/vaccines/hcp/patient-ed/conversations/downloads/vacsafe-understand-color-office.pdf.
CDC. 2015. “2014 National Immunization Survey (19-35 Months).” Accessed January 15, 2016. http://www.cdc.gov/vaccines/imz-managers/coverage/nis/child/2014-released-child-teen.html.
Diekema, Douglas S. 2014. “Personal Belief Exemptions From School Vaccination Requirements.” Annual Review of Public Health 35: 275-92.
Fefferman, Nina H., and Elena N. Naumova. 2015. “Dangers of Vaccine Refusal near the Herd Immunity Threshold: A Modelling Study.” The Lancet Infectious Diseases 15(8): 922-26.
Grabenstein, John D. 2013. “What the World's Religions Teach, Applied to Vaccines and Immune Globulins.” Vaccine 31(16): 2011-023.
Harriman, Kathleen. 2015. “2014-2015 California Measles Outbreak: It’s a Small World After All.” National Vaccine Advisory Committee. http://www.hhs.gov/nvpo/nvac/meetings/pastmeetings/2015/2014-2015_california_measles_outbreak.pdf.
McLaughlin, John M., Justin J. McGinnis, Litjen Tan, Annette Mercatante, and Joseph Fortuna. 2015. “Estimated Human and Economic Burden of Four Major Adult Vaccine-Preventable Diseases in the United States, 2013.” The Journal of Primary Prevention 36(4): 259-73.
Mississippi State Department of Health (MSDH). 2008. “National Measles Outbreaks Cause Concern.” Accessed June 2, 2016. http://msdh.ms.gov/msdhsite/_static/23,6891,341,517.html.
Opel, Douglas J., et al. 2013. “The Architecture of Provider-Parent Vaccine Discussions at Health Supervision Visits.” Pediatrics 132(6): 1037-46.
Oregon Health Authority (OHA). 2015. “Oregon's vaccine exemption rate drops 17 percent.” Accessed September 23, 2016. http://www.oregon.gov/oha/news/Pages/Oregon%E2%80%99s%20vaccine%20exemption% 20rate%20drops%2017%20percent.aspx.
Rosenthal, Brian M. 2015. “Texas Senate Health Chief Opposes Villalba Bill to Limit Vaccine Exemptions.” Houston Chronicle, February 2. http://blog.chron.com/texaspolitics/2015/02/texas-state-senators-not-eager-to-embrace-limiting-of-vaccine-exemptions.
Seither, Ranee, Kayla Calhoun, Cynthia L. Knighton, Jenelle Mellerson, Seth Meador, Ashley Tippins, Stacie M. Greby, and Vance Dietz. 2015. “Vaccination Coverage Among Children in Kindergarten — United States, 2014–15 School Year.” MMWR (Morbidity and Mortality Weekly Report) 64(33): 897-904.
Smith, David R. 2003. “The Promise of Vaccines: The Science and the Controversy.” American Council on Science and Health. Accessed June 2, 2016. http://acsh.org/news/2003/09/01/the-promise-of-vaccines-the-science-and-the-controversy/.
Smith, Philip, Sharon Humiston, Edgar Marcuse, Zhen Zhao, Christina Dorell, Cynthia Howes, and Beth Hibbs. 2011. “Parental Delay or Refusal of Vaccine Doses, Childhood Vaccination Coverage at 24 Months of Age, and the Health Belief Model.” Public Health Reports 126(2): 135-46.
Texas Department of State Health Services (TDSHS). 2016. “2015-2016 Annual Report of Immunization Status.” Accessed September 23, 2016. http://www.dshs.state.tx.us/immunize/coverage/schools.shtm.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.

