
This brief is part of a larger series that explores the intersection of gender and displacement in the Middle East and North Africa. Read the introduction to the series and explore the full set of eight briefs here.
Introduction
The health of adolescent refugees is an important yet often overlooked aspect of research and policy in the Arab world. This gap is a missed opportunity: Addressing young refugees’ health needs in adolescence can prevent negative health outcomes in the transition to adulthood and affirms their rights to equitable health access and dignified lives. For girls, this is especially important in light of their weakened social position. Adolescent girls face many challenges related to their health and well-being as they move to adulthood in the confined space of refugee camps. Among particularly vulnerable girls, health issues can multiply due to the rise of social and economic constraints inside refugee camps. Growing evidence highlights the importance of studying the health needs of refugee girls, including their physical and mental health.1
Female Palestinian refugee adolescents living in camps face enormous challenges that influence their health. Studies have shown the spatial and physical contexts of people’s lives — where and how they live — determine their health, meaning that refugee health cannot be fully understood in isolation from the spatial and physical contexts that shape and sustain health conditions and community environment. Chronic disease, mental health issues, health conditions, and behavior are all affected by spatial and physical factors such as neighborhood socioeconomics, social environment, and the physical (built) environment, all of which are amplified inside refugee camps, including Palestinian camps. Place and space take into account the social relations and social construction of a community as well as the personal experience of spatiality, temporality, and materiality that influence the process of shaping the health status of individuals, especially refugees. This study investigates the construct of space in Palestinian camps in Jordan and the West Bank, and its effect on the health of female adolescents living in these camps. We examine how place and space influence and shape the health status of refugees. To do this, we consider the social relations and social construction of these refugee communities as well as individual refugees’ personal experiences of spatiality, temporality, and materiality.
Methods
This study draws on thematic analysis2 and consists primarily of in-depth interviews and focus group discussions with adolescent girls aged 15-18 years old. There was a total of 39 interviews and 23 focus group discussions, taking place in all 19 of the Palestinian refugee camps of the West Bank as well as in the 10 camps in Jordan. In addition, 225 interviews with stakeholders — including health and education service providers and staff at women's centers and camp youth centers — were conducted in the West Bank and Jordan (respectively, 158 and 67 interviews).
Policy Context
Participants reported significant health challenges, including mental health issues. These were influenced by:
- The physical space characterized by overcrowding and lack of infrastructure.
- The social construct of space as a source of restriction, monitoring, and surveillance.
- The materiality of space in the form of deteriorating financial conditions.
Observations and experiences shared by participants point alarmingly to the consequences of the spatial context of camps: It is shown in their alienation, disempowerment, and placelessness, which have serious negative implications for refugee health, especially vulnerable girl adolescents. It is important to consider these findings in the design of future policies related to health in camp populations.
Camp Environment: Female Adolescents' Perspectives
Participants reported low levels of health — including mental well-being — characterized by chronic daily uncertainty, insecurity, and heightened vulnerability, leading to stress, reduced well-being, and somatization3 of stress and distress. Participants discussed a wide variety of factors that affect their physical and mental health. Based on their responses, these negative determinants of health and mental well-being were related to the social, physical, and economic environment. The social environment was a source of restriction and surveillance, while the physical environment was characterized by overcrowding and a lack of infrastructure. Further, many girls noted the difficult financial circumstances of camp families. These three inseparable environments (physical, social, and economic) result from the prolonged displacement of Palestinians for more than 70 years along with the continuous stigmatization of refugees, the deteriorating conditions of camps, and the lack of legal authority over the camps in Palestine and other host countries such as Jordan. These conditions and environments influence the girls’ physical health and their emotions, mood, self-esteem, and perceived well-being. The girls feel a lack of control over their own destinies, which has a negative effect on their health and mental well-being.
This issue brief focuses only on the physical and social environments.
Physical Environment and the Adolescence Transition
Many girls spoke about the physical environment in Palestinian camps, characterized by overcrowding and a lack of infrastructure. Most participants discussed the experience of living in small houses of one or two rooms, and the proximity of houses to one another, which severely limits
privacy. One girl from the Arroub camp south of the West Bank highlighted this:
"We live in the camp; all houses are close to each other. Sometimes, I know my neighbors can see me as I am sitting in my house through our windows. Our life is live-streaming to our neighbors and people in the camp.”
There is also very little space for girls to relax and get a change of scenery. Some girls said that they go up on the roof (if they have access to it) when they feel like they need to get away. The lack of privacy due to the infrastructure of the camps increases girls’ feelings of suffocation, all the more so as they are often confined to their homes.
Another key feature of the physical environment is the lack of infrastructure for girls to take part in activities, which was highlighted in both Jordan and the West Bank. They have very little space to take part in activities, especially those they consider a form of positive release like exercise. Despite the presence of women’s programming centers in the camps, activities for 15-18-year-olds are limited. In addition, girls’ movement is severely monitored and restricted, particularly in the southern and northern camps of the West Bank as well as in Jordan.
It is worth noting that in a few camps, mainly in the central West Bank — for example, the Dheisheh and Aida camps — the infrastructure and programming opportunities appear to be better than others. However, even in better-serviced camps, girls noted that there were not many opportunities for their age group since they were not considered young children. In more remote or isolated camps, the effects of the lack of infrastructure for girls were more pronounced. The lack of public services, such as waste collection and management, was another factor reiterated by participants as a key predictor of physical and mental health. They said that poor waste collection resulted
in the spread of diseases, and the view of compiled trash and waste affected their mental well-being. Participants wondered what kind of health or well-being they could have while living in such conditions. As one participant from Jenin camp in the north of West Bank noted, “It’s miserable here, there’s no security or personal safety, people are neglected, there are no services, everything is missing.”
Social Environment: Gendered Experiences
The social environment includes encounters with family and members of the wider camp community. These encounters occur in a spatial context and are subject to the general camp culture that has resulted from years of social and political exclusion of camps and camp residents from the communities surrounding them.
For many adolescent girls, in both Jordan and the West Bank, the social environment was a source of restriction and surveillance. As girls reach puberty, they are much more closely monitored by their families and communities. Girls are very cognizant of the fact that their actions will be closely monitored and that society will not be very forgiving if they make mistakes, especially within such a confined and tight-knit place. This was especially the case with relationships outside of marriage, which are highly stigmatized in camps’ conservative environments. Yet, their relationships with their immediate family members, as well as their wider family group, are critical to their health and well-being. Some participants noted that problems in the family can be a source of stress and can consequently have an adverse effect on their health.
Families played an important role in how the girls interacted with space around them — both inside homes and in the public spaces of the camp. They had a significant impact on the girls’ enrollment in school and involvement in social activities, and often determined how much mobility the girls had within the camp space.
It was important for girls to feel they were encouraged, understood, and trusted by their families and to have freedom of mobility to interact with the spaces around them. Girls who were given a greater degree of freedom by their families appeared to be well adjusted and generally had a better health status. When girls felt they were not understood by their families or did not have the space to express themselves, this had negative effects on their health and well-being, as one girl from the Baqa’a camp in Jordan explained:
“My family is strict with me, and a lot of time they tell me what to do and then outside of the house, you are forced not to go out a lot, and if I go out today then I can’t go again for a long time. You feel like they are very strict.”
The larger camp community also had a sizable influence on girls’ lives and health. While many girls spoke of positive relationships within the family, they generally had less trust in the larger community and often felt that they were under heavy scrutiny and surveillance. As one girl living in the Amman New camp expressed:
“For me, it [society] affects my mental health and I am worn out, it is possible that society can have a negative or positive effect on a person, but [our society imposes] a lot of responsibilities and pressures on us.”
The broader camp community limited the movement and mobility of girls including attending social activities, and even from playing, as one girl from the Suf camp in Jordan highlighted:
“Right, I am a child and I would like to play and would like to live my life, it’s the childhood phase let me live it, but your family, your family may understand this that you are a child and want to live your life, but the people outside influence your family and limit you.”
The public space of camps is a relational one, which means that it reflects the personal and collective belonging and identity and affects the health of individuals and communities. The experiences and encounters girls had with this public, shared space created a sense of exclusion from the camp community and space. This feeling particularly influenced their mental health, as the girls were unable to identify with any group of people that understood and supported them.
Participant Action Points
During interviews, as well as focus group discussions, participants pointed to areas where they sought change in relation to their health and life inside refugee camps — action items that they desired to have as part of interventions, recommendations, or policy reforms.
Gaps in Services. There was a gap between stakeholders and girls in terms of the services offered, as services speaking to the needs of this age group were delivered but were not reaching the target group. For example, mental health support and reproductive health services were offered, but only inside health clinics, which are generally not accessible to girls due to mobility restrictions. These services could be part of the school system, which is accessible to most girls and part of their everyday lives. Girls explained that institutions within the camps — including health centers, schools, women’s programming centers, and youth centers — rarely offered them the specific services they needed or the spaces they desired for recreational and other activities. They wanted to have summer camps, volunteering opportunities, cultural and intellectual activities, or simply school activities such as craft workshops that offered them an escape from the physical and social constraints of camps.
Gaps in Perceptions. During the in-depth interviews with stakeholders, individual girls and focus group discussions with girls, we found that there was a gap in the perceptions of stakeholders and girls, as well as communication gaps: Stakeholders’ understandings were often limited or based on minimal interactions with the girls themselves.
Fragmented Services. In addition, participants pointed out the fragmented services offered inside camps. They recommended collective and mutual activities and services be offered by all service providers inside camps. For example, health clinics and women centers could plan activities in collaboration with schools (which are accessible to most girls). This also means that the United Nations Relief and Works Agency’s (UNRWA) health, education, and relief programs, as well as local initiatives and centers, should work together in planning and implementing services and interventions that are coherent and complementary. Participants specifically wanted to have activities targeting them and their needs, as well as recreational activities that allow them to grow, learn, and interact with the larger camp community. This was a key priority.
Family Education. Girls also recommended having educational and informational sessions for their families, primarily their mothers, to better accommodate their needs and to gain some privacy inside the home. They sought improved mobility and interaction in the broader camp space so they could take part in social and recreational activities.
Image 1 — Jarash Palestinian Refugee Camp in Jordan 2018

Image 2 — Irbid Palestinian Refugee Camp in Jordan in 2018

Other Factors to Consider
Social Isolation of Camps. There is also a broader issue to confront: Although camps are not physically isolated from their surrounding neighborhoods, they are socially isolated. This has resulted in the formation of tight-knit social clusters inside camps, which over time became stereotyped as spaces of illegitimacy, rebellion, and resistance. To counter this isolation and stereotyping, we recommend planning and implementing activities that integrate camp residents with the surrounding communities — for example, policies to encourage participation of camp residents in work outside the camp and in public spaces such as public schools.
No Body with Legal Authority. Another significant factor is that there is no body with legal authority over the camps. This means there is no body legally responsible for the protection of rights and basic infrastructure services inside camps including paved streets, supply of water and electricity, waste management, and the establishment of public spaces that host youth, including female adolescents. While the United Nations Relief and Works Agency for Palestine Refugees in the Near East is currently providing a number of these services, they are not legally obliged to do so, and camps are generally excluded from public reforms or infrastructural projects. This has resulted in the continuing deterioration of camp infrastructure.
Recommendations
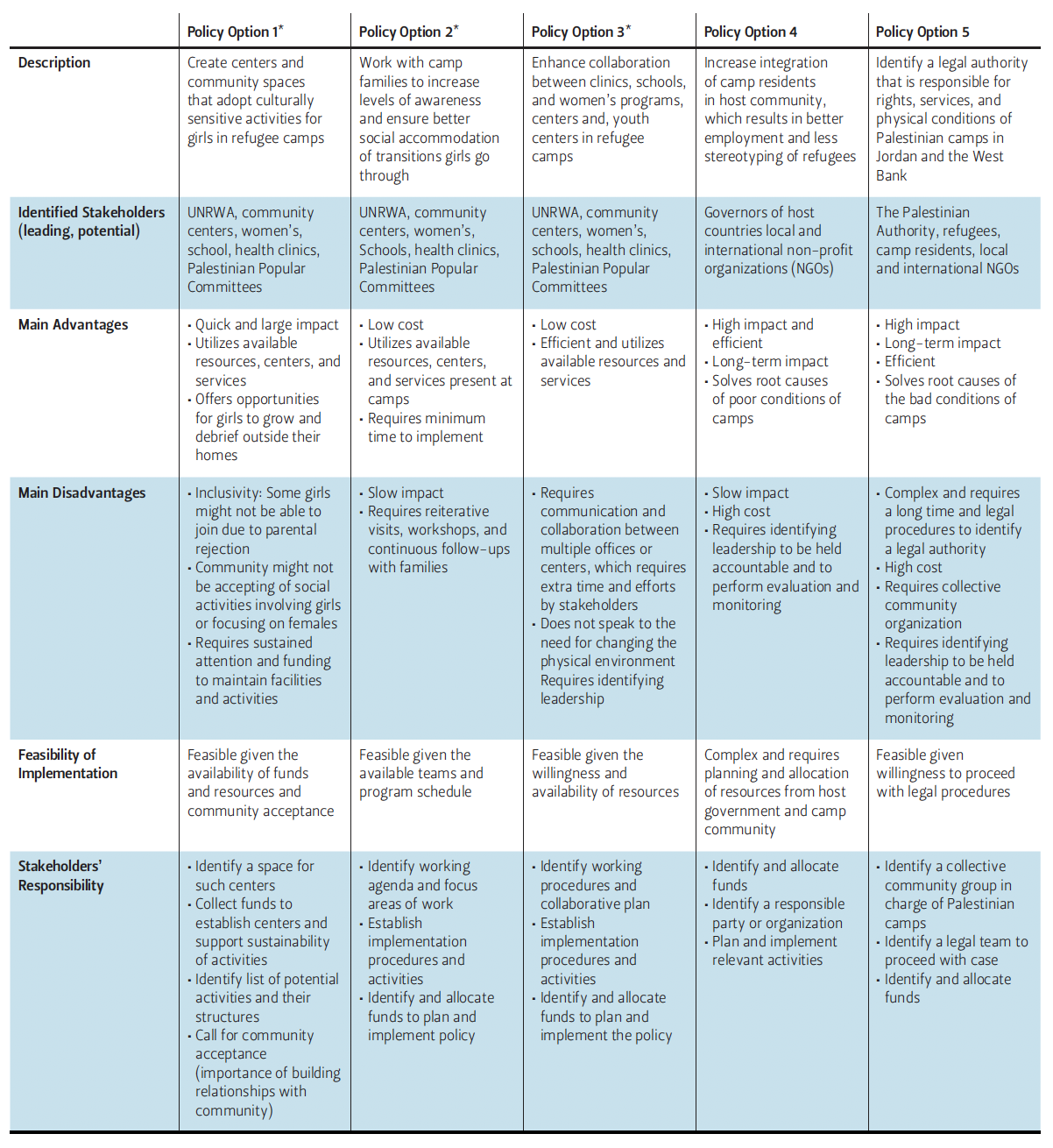
Table 1 presents the main recommendations and includes details about the advantages,
disadvantages, and feasibility of each recommendation.
Table 1 — Policy Recommendations to Improve the Health of Palestinian Refugee Girls
Acknowledgments
The authors would like to thank UNRWA for their support throughout the project. This work was carried out with the aid of a grant from the International Development Research Centre (IDRC), Ottawa, Canada. The views expressed herein do not necessarily represent those of IDRC or its Board of Governors.
References
Abourahme, Nasser. “The Camp.” Comparative Studies of South Asia, Africa and the Middle East 40, no. 1 (2020): 35–42. https://doi. org/10.1215/1089201X-8186016.
Abourahme, Nasser. “Assembling and Spilling-Over: Towards an ‘Ethnography of Cement’ in a Palestinian Refugee Camp.” International Journal of Urban and Regional Research 39, no. 2 (March 2014): 200–217. https://doi.org/10.1111/1468-2427.12155.
Abourahme, Nasser. “Spatial Collisions and Discordant Temporalities: Everyday
Life between Camp and Checkpoint.” International Journal of Urban and Regional Research Volume 35, no. 2 (March 2011): 200–217. https://doi.org/10.1111/j.1468-2427.2010.01034.x.
Anera, Who are Palestinian Refugees? The Olive Press Blog, August 19, 2022,. https://www.anera.org/blog/who-are-palestinian-refugees/.
Baar, Johanna, Matthias Romppel, Ulrike Igel, Elmar Brähle and Gesine Grande. “The Association Between Physical Environment and Health: Indicating the Direction of Effects Using German Panel Data.” International Journal of Occupational and Environmental Health 22, no. 1 (2016). https://doi.org/10.1080/10773525.2015.1106074.
Dyck, Isabel, and Parin Dossa. “Place, Health and Home: Gender and Migration in the Constitution of Healthy Space.” Health & Place 13, no. 3 (September 2007): 691–701.
Hanafi, Sari. “Governing Palestinian Refugee Camps in the Arab East: Governmentalities in Search of Legitimacy.” Issam Fares Institute for Public Policy and International Affairs. Working Paper Series 1, October 2010, American University: Beirut.
Hughes, J, and A.P. McCauley. “Improving the Fit: Adolescents’ Needs and Future Programs for Sexual and Reproductive Health in Developing Countries.” Studies in Family Planning 29, no. 2 (June 1998): 233–45.
Knudsen, Are, and Sari Hanafi eds. Palestinian Refugees: Identity, Space, and Place in the Levant (Routledge, 2011).
Netto, Vinicius. “Practice, Communication and Space: A reflection on the Materiality of Social Structures.” Ph.D. diss, 2007, University of London. https://discovery.ucl.ac.uk/id/eprint/5060/.
Rickard-Brideau, Carol. “The Connection Between Space and Wellness,” November 26, 2018, https://www.littleonline.com/insights/theconnection-between-space-andwellness-2/.
Sajdi, Jude, Aida Essaid, Clara Miralles Vila, Hala Abu Taleb, Majed Abu Azzam and Agnieszka Malachowska. “‘I Dream of Going Home’: Gendered Experiences of Adolescent Syrian Refugees in Jordan’s Azraq Camp.” European Journal of Development Research (2021). https://doi.org/10.1057/s41287-021-00450-9.
Senderowitz, Judith. Making Reproductive Health Services Youth Friendly. Focus on Young Adults, Research, Program and Policy Series (February 1999). https://pdf.usaid.gov/pdf_docs/PNACK127.pdf.
Vis, Benjamin. Built Environments, Constructed Societies: Inverting Spatial Analysis (Sidestone Press, 2009).
Woolf, Steven, and Laudan Aron, eds. “Physical and Social Environmental Factors“ in U.S. Health in International Perspective: Shorter Lives, Poorer Health (Washington, D.C.: National Academies Press, 2013). https://www.ncbi.nlm.nih.gov/books/NBK154491/.
Endnotes
1. See Hani Mowafi, “Conflict, displacement and health in the Middle East,” Global Public Health 6 no. 5 (2011): 472–487, https://doi.org/10.1080/17441692.2011.570358; Maren M. Hawkins et al., “Promoting the health of refugee women: A scoping literature review incorporating the social ecological model,” International Journal for Equity in Health 20, no. 45 (2021), https://doi.org/10.1186/s12939-021-01387-5; Selcuk R. Sirin and Lauren Rogers-Sirin, The Educational and Mental Health Needs of Syrian Refugee Children (Washington, D.C.: Migration Policy Institute, 2015), https://
www.migrationpolicyinstitute-europe.com/sites/default/files/publications/FCD-Sirin-Rogers-FINAL.pdf; World Health Organization, “Common Health Needs of Refugees and Migrants: Literature Review” (2021), https://apps.who.int/iris/handle/10665/346743.
2. Thematic analysis is “a qualitative research strategy for identifying, analyzing, and reporting identifiable patterns or themes within data.” See APA Dictionary, https:// dictionary.apa.org/thematic-analysis.
3. Somatization is the “conversion of a mental state (such as depression or anxiety) into physical symptoms, also the existence of physical bodily complaints in the absence of a known medical condition.” See Merriam Webster, https://www.merriam-webster.com/dictionary/somatization.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.

