
Executive Summary
Purpose
Roughly half of the U.S. population now lives in a state that permits recreational cannabis use and sales. Still, the criminal legal system continues to play a primary role in determining who receives treatment for cannabis use. It remains the single largest treatment referral source, and in 2019 more than 100,000 people who were admitted to treatment for cannabis use were referred by a legal entity.[1]
This raises questions regarding the extent to which individuals who interact with the legal system are monitored and punished for cannabis use in the post-legalization era. Moreover, the issue has not been addressed by state legalization measures.
We examined trends in legal system referrals to treatment for cannabis use in legal and nonlegal states from 2007 to 2019. We also tested the relationship between recreational cannabis legalization and legal system treatment referrals for Black, Hispanic, and white adults and juveniles.[2]
Why This Matters
The legal system’s practice of requiring individuals to participate in drug treatment warrants scrutiny because of its potentially negative and long-lasting consequences. While mandated treatment may be appropriate in some cases, the legal system often requires treatment participation from individuals who do not meet the criteria for a substance use disorder, and it does a poor job of connecting those who do have substance use disorders with appropriate care.[3]
The legal system’s limited efficacy in this arena is problematic because mandated treatment carries the possibility of additional legal consequences if program expectations are not met. The harmful effects of legal involvement include fewer education and employment prospects, reduced earning potential, destabilized family structures, negative mental and physical health outcomes, and diminished quality of life. Communities of color are disproportionately targeted by drug enforcement and disproportionately impacted by its collateral consequences.
Recreational cannabis legalization (RCL) is intended to remedy, in part, the harmful and racially disparate effects of cannabis prohibition. However, the continuation of compulsory treatment for cannabis use, and the legal involvement it entails, is a potential pathway through which the systemic harms and inequities of cannabis prohibition can persist. The problematic nature of this arrangement is enhanced when it occurs alongside a commercial cannabis industry that profits from greater levels of cannabis use.
Methods
Using data from the Treatment Episode Data Set-Admissions (TEDS-A) for 2007 to 2019, we created variables for state-level rates of legal system-referred cannabis treatment admissions for Black, Hispanic, and white adults and juveniles. We compared rate trends across populations and conducted staggered difference-in-difference and event analyses to determine whether RCL is associated with a decline in legal system referrals to treatment for cannabis use.
Findings
In legal states, the average cannabis treatment admissions rate declined 57.19% from 2007 to 2019, compared to a 41.06% decline in nonlegal states over the same period. Admissions rates declined for all populations of study; however, RCL was not associated with these declines when controlling for sociodemographic factors.
Black juveniles had the highest average admissions rate (20.16 per 10,000), followed by Hispanic juveniles (12.35), Black adults (9.18), white juveniles (7.58), Hispanic adults (3.42), and white adults (1.66). On average, juveniles had higher admissions rates and experienced greater percentage declines in these rates compared to their adult counterparts in both legal and nonlegal states.
Black and Hispanic populations experienced smaller percentage declines in admissions rates than their white counterparts. Racial/ethnic disparities in admissions rates increased in both legal and nonlegal states, with greater increases in legal states. In 2019, racial/ethnic disparities were higher in legal states than nonlegal states for all groups except Black juveniles.
Implications
Our findings suggest that RCL has not fundamentally altered the legal system’s practice of requiring defendants who use cannabis to receive drug treatment, nor has it reduced racial and ethnic disparities in referral practices. White adults and juveniles experienced steeper declines in admissions rates than Black and Hispanic adults and juveniles. As a result, racial and ethnic disparities in admissions rates grew in both legal and nonlegal states, with a larger increase in legal states. These findings, coupled with prior research on RCL and cannabis arrest trends as well as evidence of disparate opportunities in nascent cannabis markets, suggest that Black, Hispanic, and youth populations are less likely to benefit from cannabis reform.
Based on our findings and the research to date, we recommend the following:
- Enact cannabis reform policies that explicitly target legal system features beyond arrest and prosecution.
- Adopt education reforms that reduce school systems’ reliance on punitive disciplinary measures to respond to students’ use of alcohol and other drugs.
- Implement regulatory policies that discourage heavy consumption of high-potency THC products to reduce the prevalence of cannabis use disorders in RCL states.
- Invest resources for addressing substance use, like opioid settlement funds, into school- and community-based initiatives rather than law enforcement programs.
Introduction
As of November 2023, 24 states and the District of Columbia have legalized recreational cannabis use for adults 21 and older.[4] Recreational cannabis legalization (RCL) is popular with the American public for many reasons, including its potential to reduce the excessive and racially disparate use of the criminal legal system to enforce cannabis prohibition.
RCL has been accompanied by a significant drop in cannabis possession arrests. This is a welcome development, but it does not mean that legal consequences for using cannabis have disappeared. Individuals are still arrested for violating remaining cannabis laws, and thousands of legal-state residents still have criminal records related to cannabis that create employment and quality-of-life obstacles. Individuals who use cannabis and who become involved in the legal system may also still face legal consequences for their cannabis use.
Historically, the criminal legal system has taken a zero-tolerance approach to cannabis use. Those charged with cannabis-related offenses were typically required to participate in drug treatment as a condition of probation or in lieu of incarceration, even if they did not have a cannabis use disorder. Non-cannabis offenses, like theft or domestic violence, could also trigger mandatory treatment if the individual’s cannabis use was discovered by a court or probation department.
Today, courts and probation departments in RCL states may still require legal system-involved individuals who use cannabis to receive drug treatment. The legalization of cannabis for recreational use and commercial sale warrants a reconsideration of such compulsory treatment requirements. This issue has not been addressed by state legalization initiatives.
At first glance, requiring legal system-involved individuals who use cannabis to participate in drug treatment may appear fairly benign. But the legal system is ill-suited to identify individual treatment needs. It often refers to treatment individuals who do not meet the criteria for a substance use disorder, an error that occurs more often for Black individuals.[5] It is also not effective at connecting those who do have substance use disorders with the appropriate care.[6]
The legal system’s limited efficacy in this area is problematic because mandated treatment, in addition to costing an individual time and money, carries the possibility of further legal consequences if program expectations are not met. The harmful effects of legal involvement include fewer education and employment prospects, reduced earning potential, destabilized family structures, negative mental and physical health outcomes, and diminished quality of life.
Communities of color are disproportionately targeted by drug enforcement and are disproportionately impacted by its collateral consequences. RCL is intended to remedy, in part, the harmful and racially disparate effects of cannabis prohibition. Compulsory treatment, and the legal involvement it entails, is a potential pathway through which the harms and systemic inequities of cannabis prohibition can persist.
This report reviews findings from our analysis of legal system referrals to cannabis treatment in legal and nonlegal states.[7] We find that recreational cannabis legalization has not impacted legal system referral practices or reduced racial and ethnic disparities in referral rates. We conclude with recommendations for policymakers.
Background
The “war on drugs” caused an explosive growth in drug arrests. In 1980, there were an estimated 580,900 drug arrests in the United States. By 2007, this figure had swelled to 1.84 million, nearly half of which were cannabis related.[8] As arrest rates rose, so did referrals to drug treatment. Between 1992 and 2008, the number of adolescents and young adults in treatment for cannabis use increased 344%.[9]
Today, the legal system is the largest referral source to treatment for cannabis use. In 2019, roughly half (49.2%) of the 208,843 individuals admitted to treatment for cannabis were referred through the legal system.[10] Black individuals are overrepresented in cannabis treatment referrals, accounting for 35% of admissions, despite similar use rates across demographic groups.[11]
Several studies have consistently found RCL to be associated with declines in cannabis-related arrests. However, this relationship varies depending on the population and place in question.[12] RCL is associated with a decline in cannabis possession arrests for adults but not for juveniles.[13] While arrests declined for Black and white populations post-legalization, in many cases racial disparities have persisted and, in some states, increased.[14]
Cannabis arrests have also declined in nonlegal states, and a number of factors other than commercial legalization — including macro-level social and political changes and local-level shifts in enforcement patterns and priorities — have likely influenced arrest trends.[15]
Thus, while RCL may be reducing the legal system’s cannabis footprint, features of prohibition endure, most notably the continued racial disparities in remaining cannabis enforcement practices.
Our Study
We sought to build on research examining the impact of RCL on arrest trends by looking at the relationship between legalization and legal system referrals to treatment for cannabis use. While arrest data measure street-level police responses to cannabis-related activity, “referrals to treatment capture activity of legal system entities, including courtroom actors, diversionary programs, and probation departments, that handle cases after an arrest has been made.”[16] These actors have considerable discretion in determining individual case outcomes and can decide whether to require an individual to participate in a treatment program for cannabis use as a condition of a more lenient sentence. Thus, evaluating trends in legal system treatment referrals “adds to research on arrests to provide a more complete picture of how the criminal legal system as a whole responds to cannabis use post-reform.”[17]
We analyzed data from the Treatment Episode Data Set-Admissions (TEDS-A), compiled by the Substance Abuse and Mental Health Services Administration (SAMHSA) for the period between 2007 and 2019. TEDS-A provides information on admissions to publicly funded substance-use treatment facilities and includes data on treatment referral source, primary substance for referral, and client demographics. We focused on referrals originating from the criminal legal system, for which the TEDS-A includes the following categories: probation and parole, diversionary programs, federal and state courts, the formal adjudication process, DUI courts, prisons, and other recognized legal entities. We examined state-level legal system-referred admissions rates for Black, Hispanic, and white adults (18 years and older) and for Black, Hispanic, and white juveniles (12 to 17 years old).
Methodology
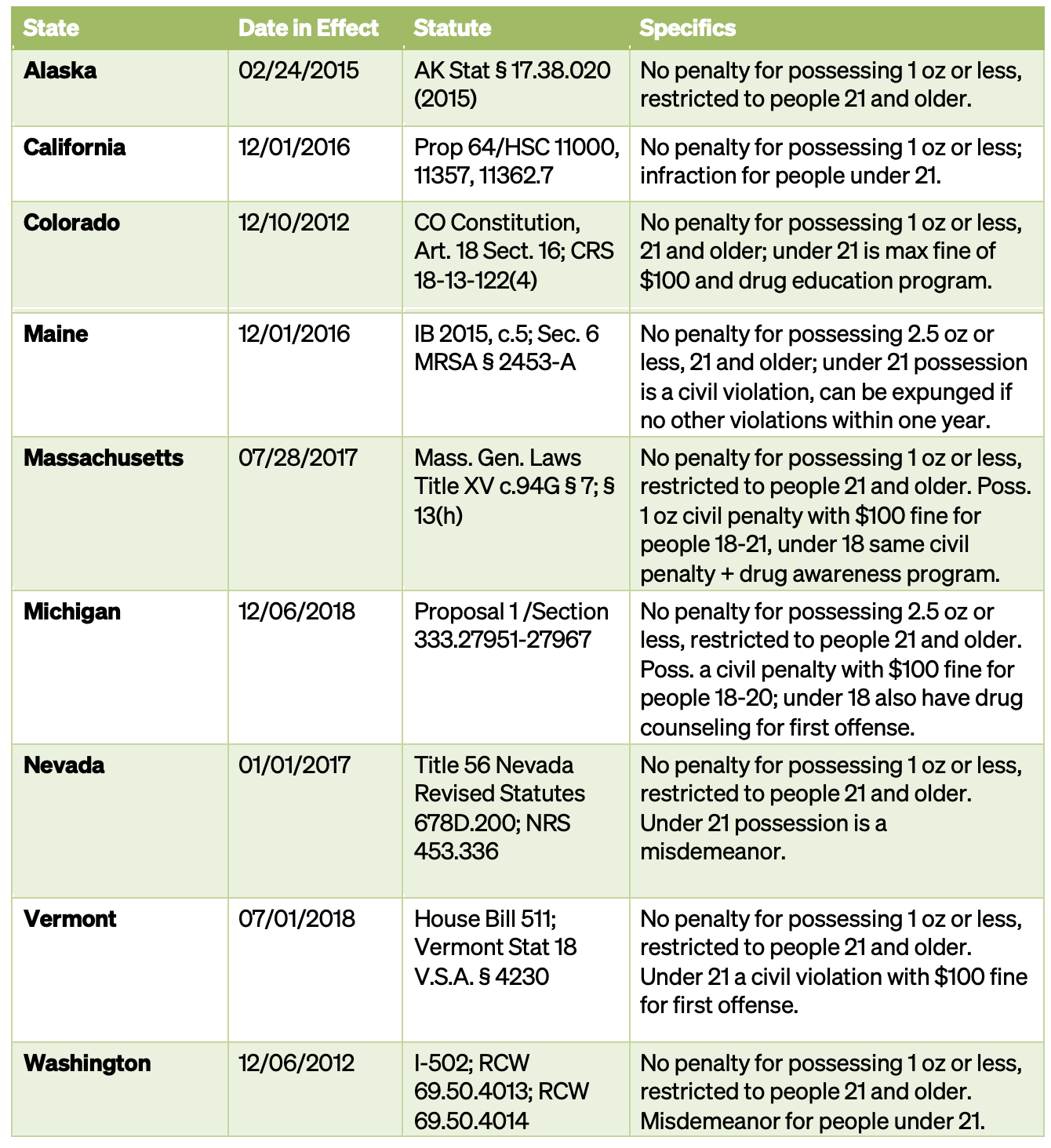
Our independent variable was state legalization of cannabis for recreational use, defined as the removal of all civil and criminal penalties for possession of cannabis (Table 1). This was treated as a dichotomous variable, where “1” denotes legalization and “0” indicates no change. Coding was based on the date that possession became legal. States with limits on the amount of cannabis that is legal to possess and states that had not yet permitted sales or home cultivation were coded as legal states.
Table 1 — State Adult-Use Cannabis Legalization Policies
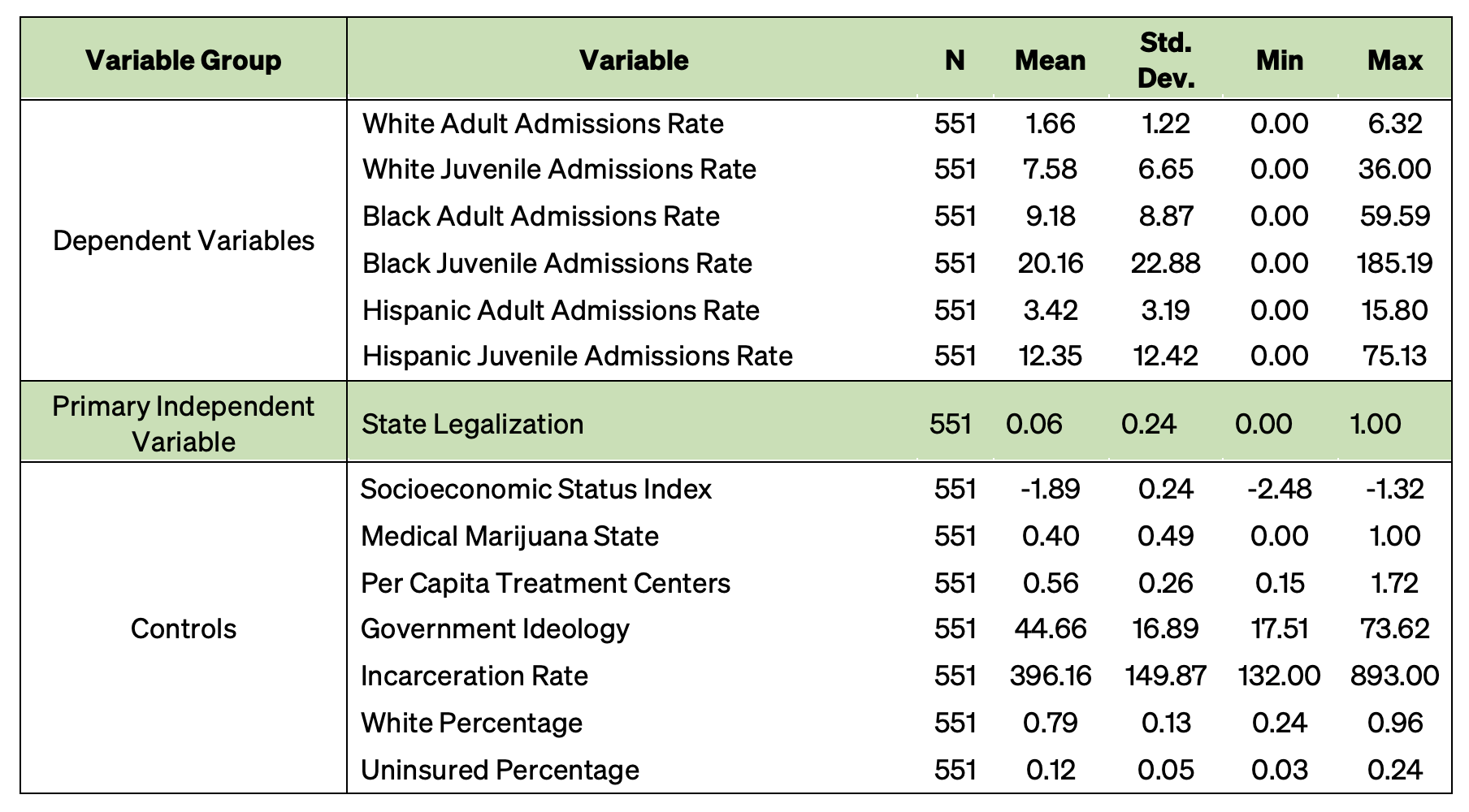
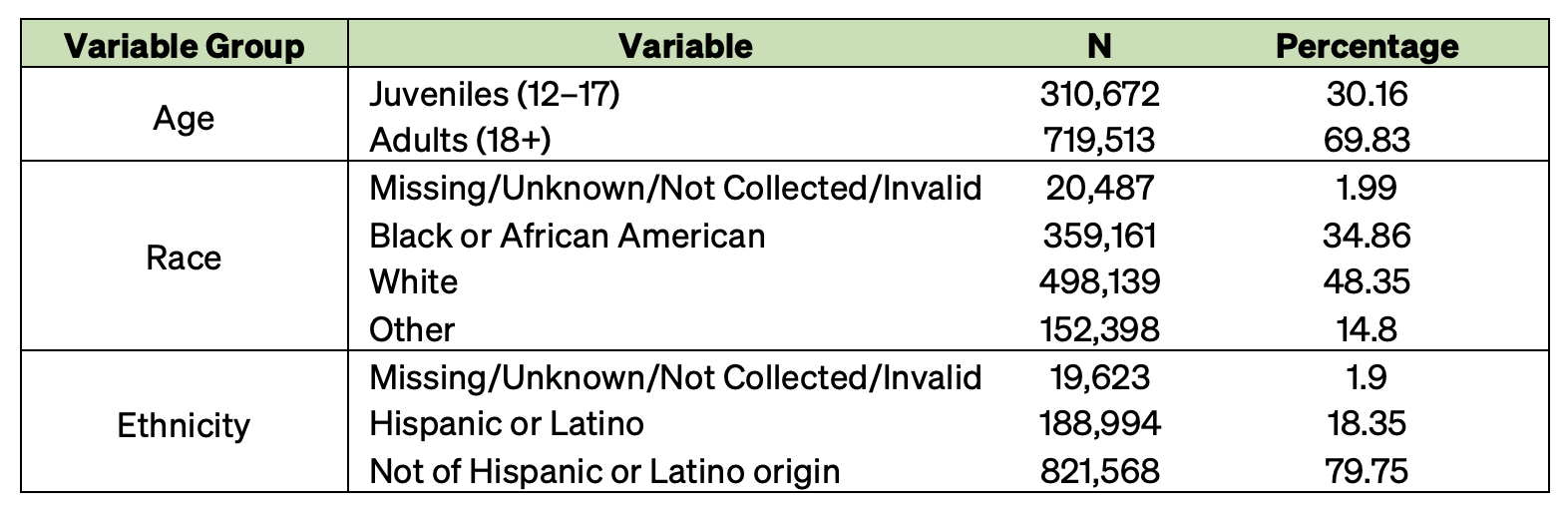
Our dependent variables were the state-level rates of legal system-referred admissions to treatment for cannabis as the primary substance of use. We used TEDS-A data for first-time admissions to treatment for the period 2007 to 2019, for a total of 1,030,185 individual observations. The individual observations were used to create the state rates of legal system-referred treatment admissions for cannabis use by age and race/ethnicity. We calculated separate admissions rates for Black, Hispanic, and white adults (18 years and older) and for Black, Hispanic, and white juveniles (12 to 17 years old). To calculate these rates, we totaled the number of individual observations for each state by year, divided by the relevant state population, and multiplied by 10,000. This produced a total of 551 state-level observations for the period from 2007 to 2019.
We controlled for the following variables: 1) percentage of white population, 2) rate of substance treatment facilities per 10,000 residents, 3) percentage of uninsured population, 4) an index for socioeconomic disadvantage that includes measures for household poverty rate, percentage of female-led households with children, percentage of individuals with a bachelor’s degree or higher, and percentage of owner-occupied housings, 5) state government ideology, 6) state incarceration rates, and 7) a dummy variable indicating whether a state has legalized cannabis for medical use.[18]
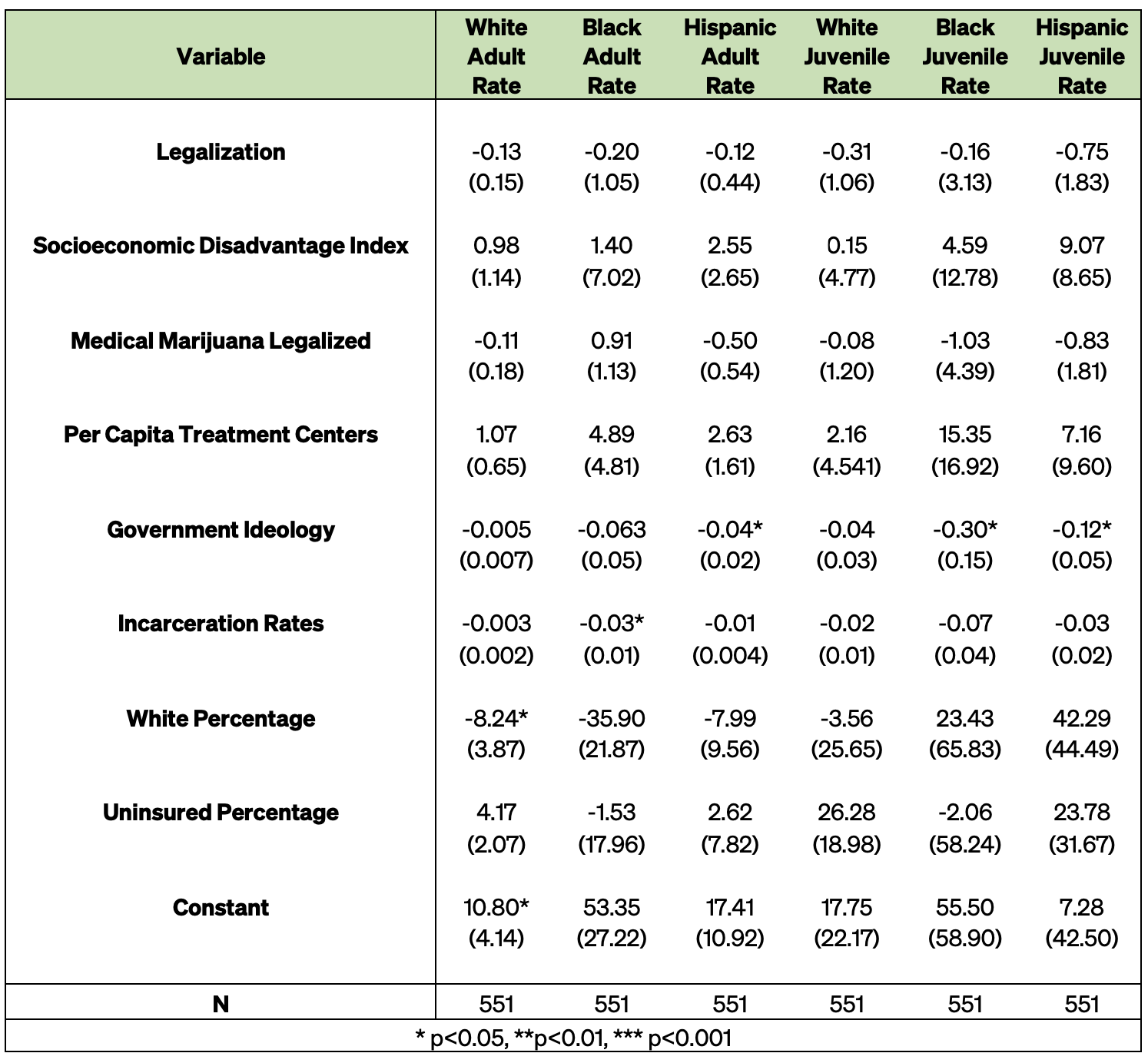
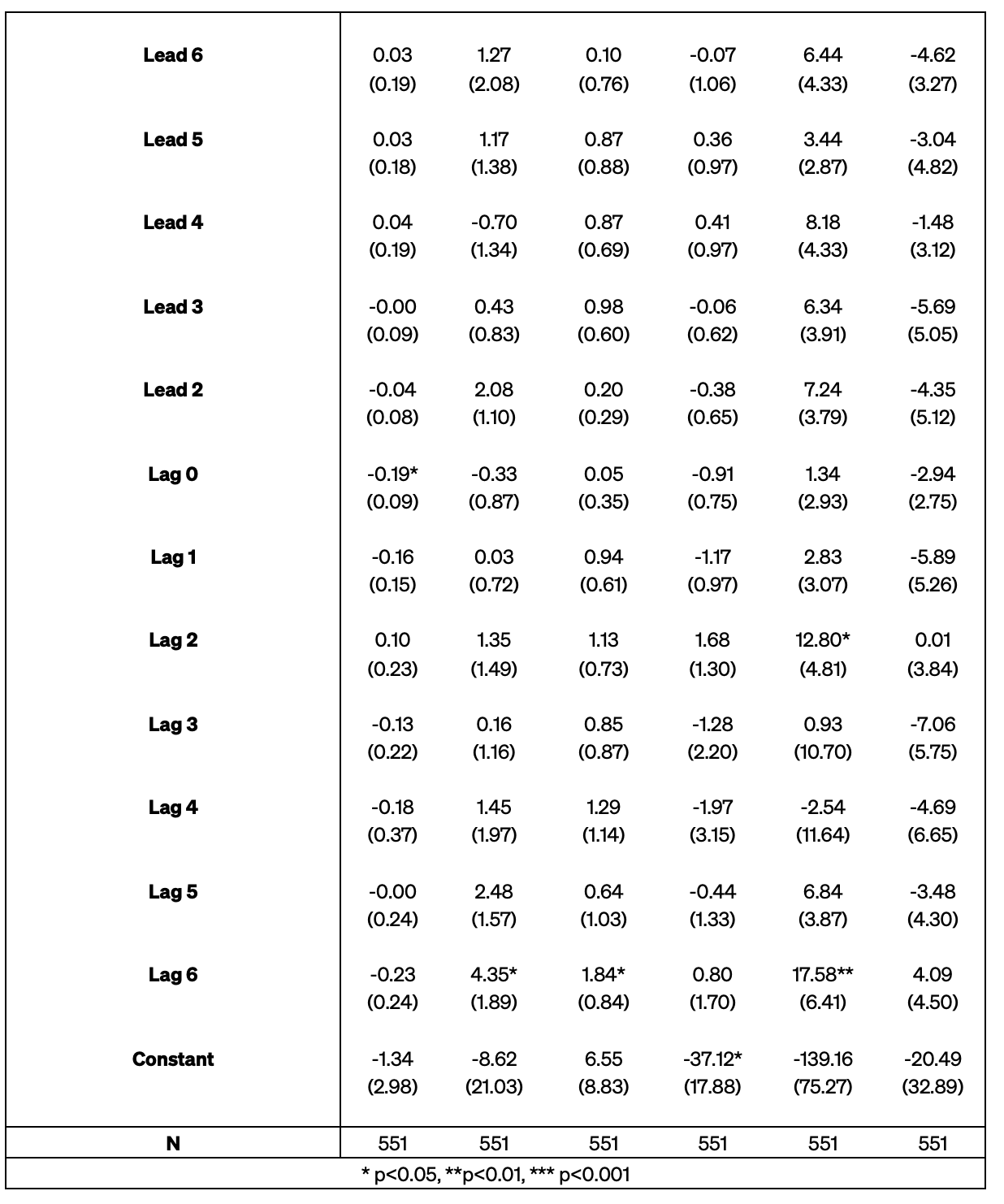
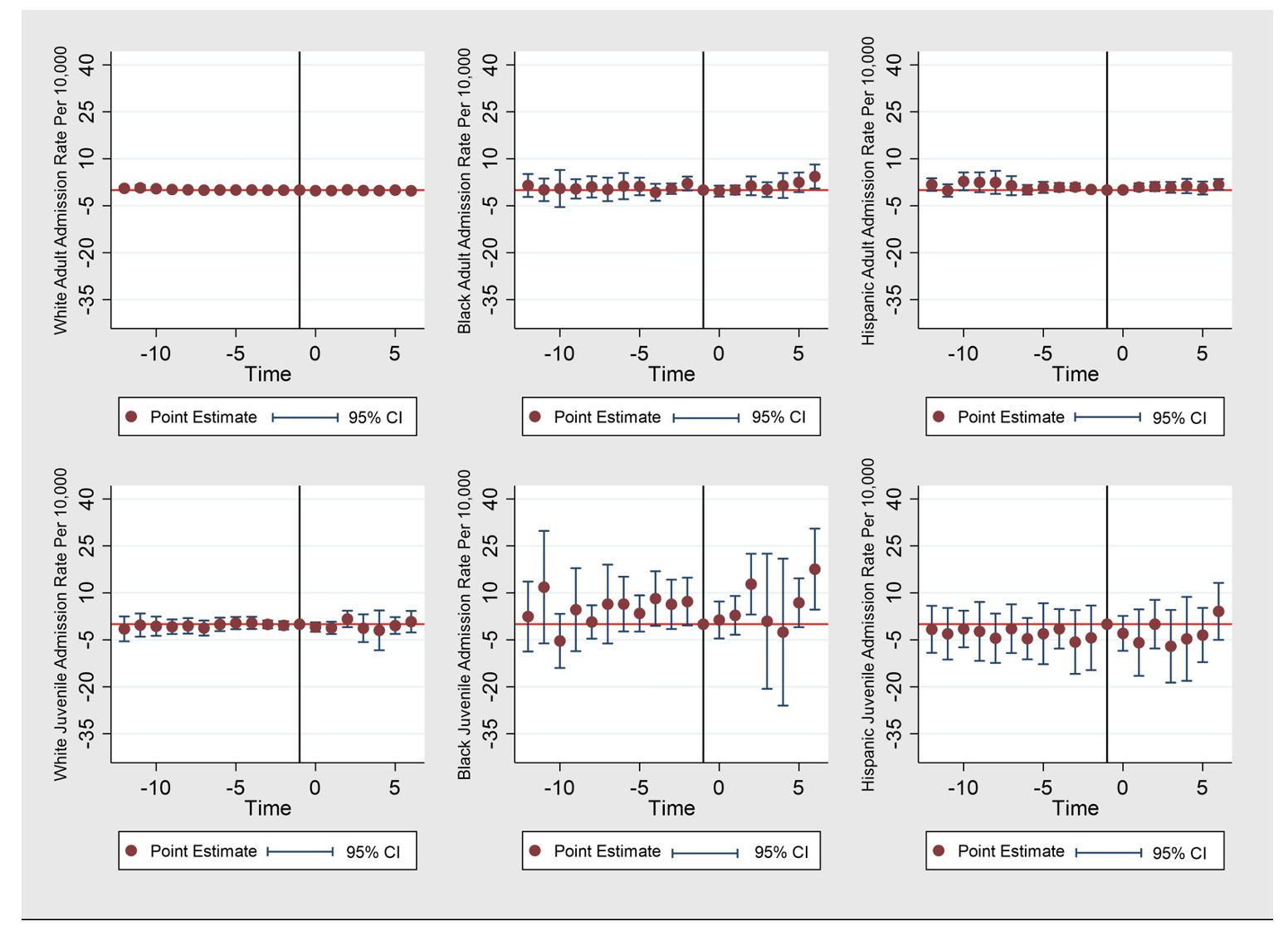
We conducted our analysis in five steps. First, we calculated descriptive statistics to understand the nature of our variables (Appendix). Second, we graphically compared average annual admissions trends between legal and nonlegal states by racial/ethnic group and age. Third, to better capture potential disparities, we plotted the relative differences in admissions rates between white and Black adults, white and Hispanic adults, white and Black juveniles, and white and Hispanic juveniles. Fourth, we used staggered difference-in-difference to determine whether legalization had a significant impact on treatment referral trends, with separate models estimated for Black, Hispanic, and white adults and juveniles.[19] The models were carried out using fixed effects with errors clustered at the state level. Lastly, we conducted a series of event panel analyses with fixed effects and clustered errors at the state level.
Like difference-in-difference, event analysis is used to determine the effects of a policy change over time. However, the event analysis better accounts for heterogeneity in policy implementation time by creating a standard baseline around which to test the impact of the treatment variable. This allows us to examine more clearly trends in cannabis admissions in the years preceding and following legalization in states that enacted reforms in different years. All analyses were conducted using the statistical analysis software STATA 16.[20]
Findings
Overall Trends
- For the study period (2007–19), the average legal system-referred admissions (hereafter, “admissions”) rate for the total population was 2.75 per 10,000 residents, with nonlegal states having a higher average rate (2.88) than legal states (2.18).
- Black juveniles had the highest average admissions rate (20.16 per 10,000), followed by Hispanic juveniles (12.35), Black adults (9.18), white juveniles (7.58), Hispanic adults (3.42), and white adults (1.66).
- In legal states, the average admissions rates declined 57.19% from 2007 to 2019. Declines started prior to legalization in all states. The size of the decline ranged from 11.5% in Colorado to 99.7% in Washington (Figure 1).
- In nonlegal states, the average admissions rate declined 41.06% from 2007 to 2019.
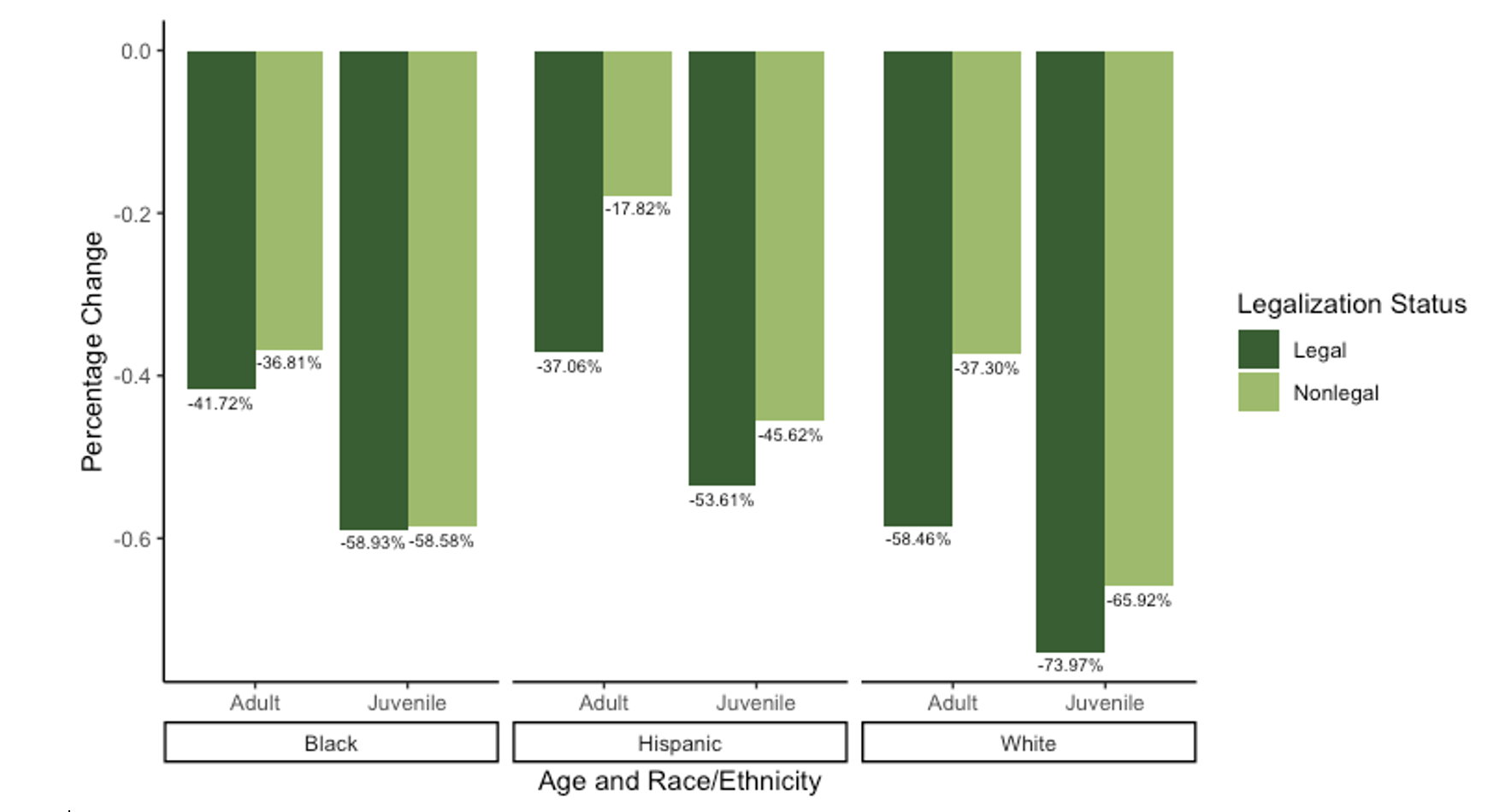
- The size of the decline was greater in legal than nonlegal states for all populations except Black juveniles, for whom average admissions rates declined roughly 59% in both legal and nonlegal states (Figure 2).
- White juveniles experienced the greatest declines in both legal and nonlegal states, followed by Black juveniles, white adults, Hispanic juveniles, Black adults, and Hispanic adults (Figure 2).
- While cannabis treatment admissions rates for all groups fell during the study period, legalization was not associated with these declines when controlling for sociodemographic factors.
- Higher uninsured rates were associated with higher admissions rates for all groups (event analysis).
- Higher levels of socioeconomic disadvantage were associated with higher admissions rates for Hispanic adults and juveniles (event analysis).
- Higher levels of government conservatism were associated with higher admissions rates for Black juveniles and Hispanic adults and juveniles (difference-in-difference) analysis.
- Higher incarceration rates were associated with lower admissions rates for Black adults (difference-in-difference) analysis (Appendix).
Figure 1 — Cannabis Treatment Admissions Trends in RCL States
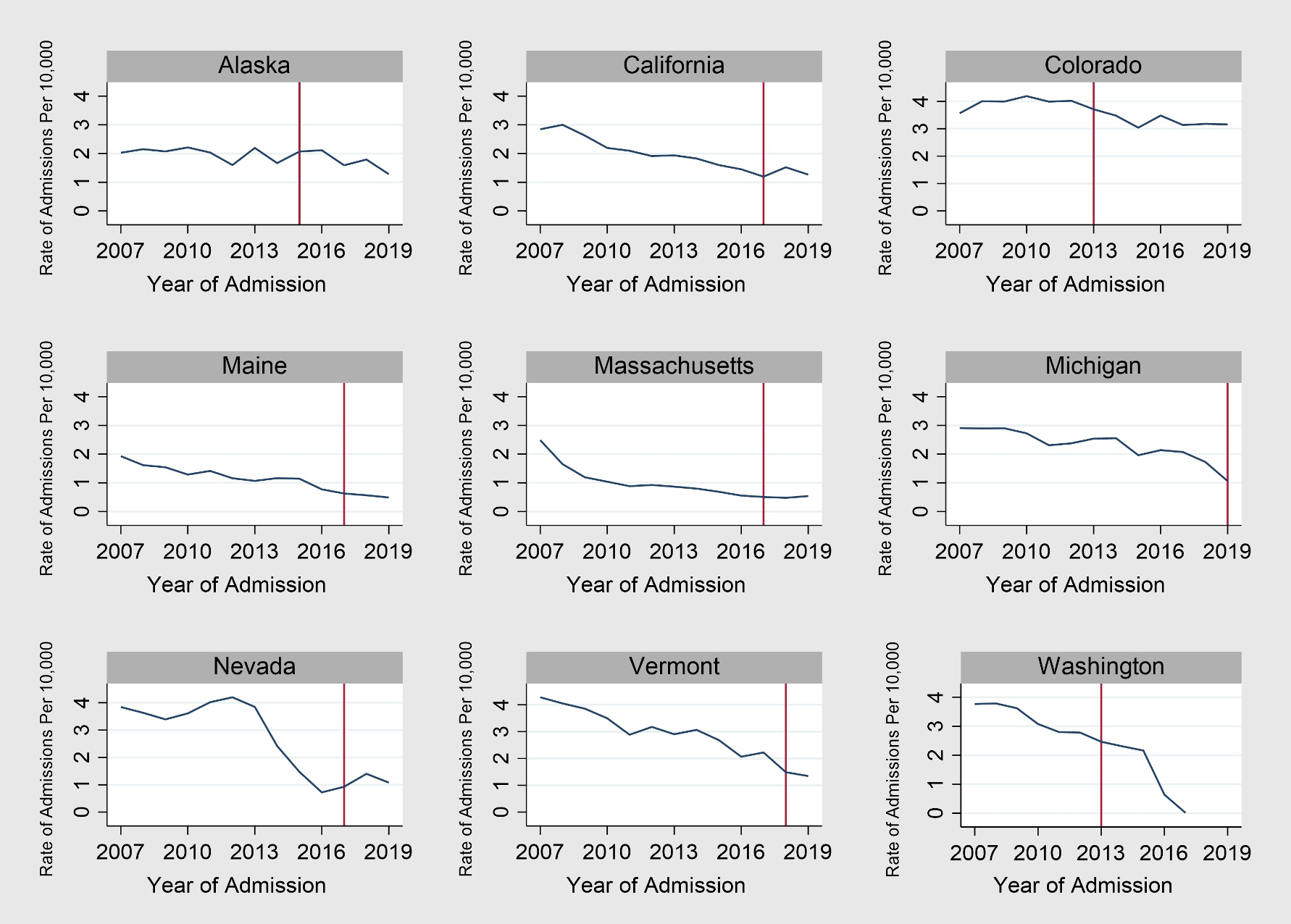
Note: Red line marks the year cannabis was legalized.
Figure 2 — Size of Decline in Admissions Rates, 2007–19
Age Disparities
- On average across all states, juveniles had higher admissions rates than their racial/ethnic adult counterparts.
- Juvenile populations experienced greater percentage declines in admissions rates than their adult counterparts in both legal and nonlegal states (Figure 2).
- Age disparities declined for all groups in both legal and nonlegal states over the study period.
- In 2019, white juveniles were admitted to treatment at a rate 2.9 times higher than white adults in legal states and at a rate 2.84 times higher in nonlegal states.
- In 2019, Black juveniles were admitted to treatment at a rate 1.44 times higher than Black adults in legal states and at a rate 2.14 times higher than Black adults in nonlegal states.
- In 2019, Hispanic juveniles were admitted to treatment at a rate 2.19 times higher than Hispanic adults in legal states and at a rate 2.82 times higher than Hispanic adults in nonlegal states.
- Age disparities fell more sharply in nonlegal states than legal states from 2007 to 2019 (Figure 3).
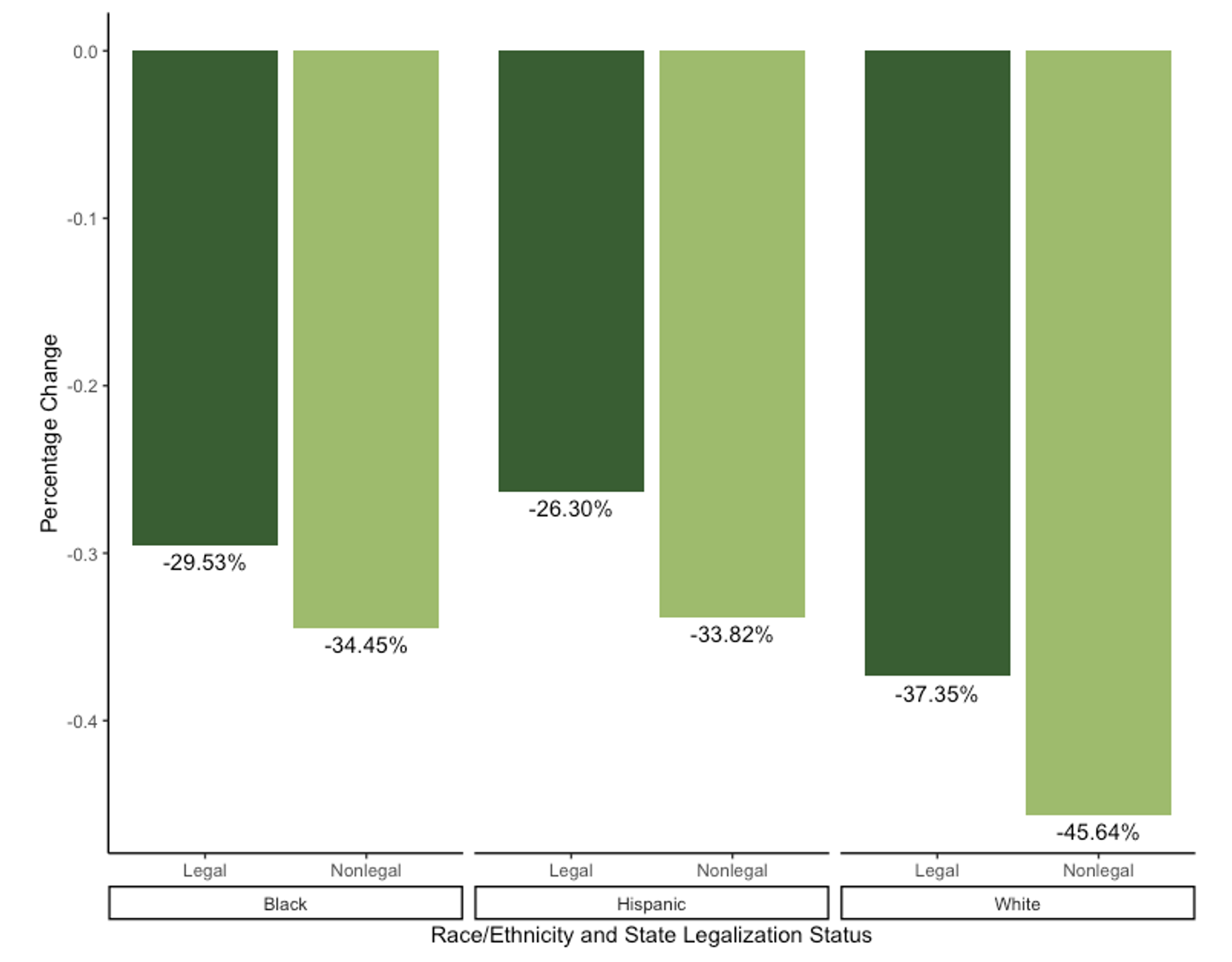
- The white juvenile/adult disparity decreased 37% in legal states and 46% in nonlegal states. The Black juvenile/adult disparity decreased 29% in legal states and 34% in nonlegal states, and the Hispanic juvenile/adult disparity decreased 26% in legal states and 34% in nonlegal states.
Figure 3 — Change in Age Disparities in Admissions Rates, 2007–19
Racial/Ethnic Disparities
- On average across all states, Black and Hispanic admissions rates were higher than white admissions rates.
- Black and Hispanic populations experienced smaller percentage declines in admissions rates than their white counterparts (Figure 2).
- Racial/ethnic disparities in admissions rates increased in both legal and nonlegal states, with greater increases in legal states (Figure 4).
- The Hispanic/white juvenile disparity increased 78% in legal states and 60% in nonlegal states. The Hispanic/white adult disparity increased 51% in legal states and 31% in nonlegal states. The Black/white juvenile disparity increased 58% in legal states and 22% in nonlegal states. The Black/white adult disparity increased 40% in legal states and held stable in nonlegal states (+.79%).
- In 2019, disparities were higher in legal states for all groups except Black juveniles (Figure 5).
- In 2019, Black adults were admitted to treatment at a rate 6.67 times higher than white adults in legal states and at a rate 4.97 times higher than white adults in nonlegal states.
- In 2019, Black juveniles were admitted to treatment at a rate 3.31 times higher than white juveniles in legal states and at a rate 3.75 times higher in nonlegal states.
- In 2019, Hispanic adults were admitted to treatment at a rate 3.0 times higher than white adults in legal states and at a rate 1.95 times higher in nonlegal states.
- In 2019, Hispanic juveniles were admitted to treatment at a 2.28 times higher rate than white juveniles in legal states and at a 1.93 times higher rate in nonlegal states.
Figure 4 — Change in Racial/Ethnic Disparities, 2007–19
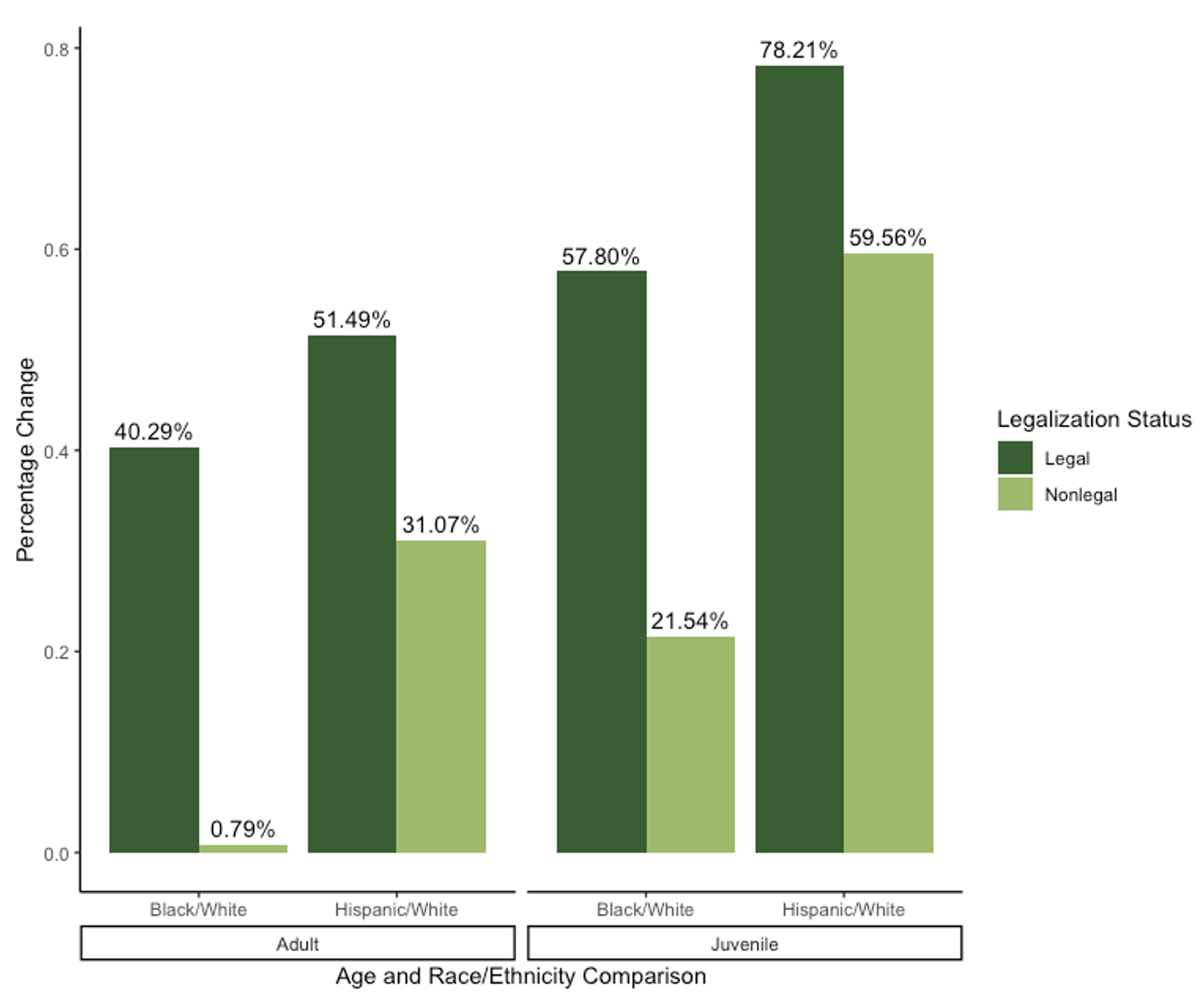
Figure 5 — Size of Disparity in Admissions Rates by Race and Ethnicity in 2019
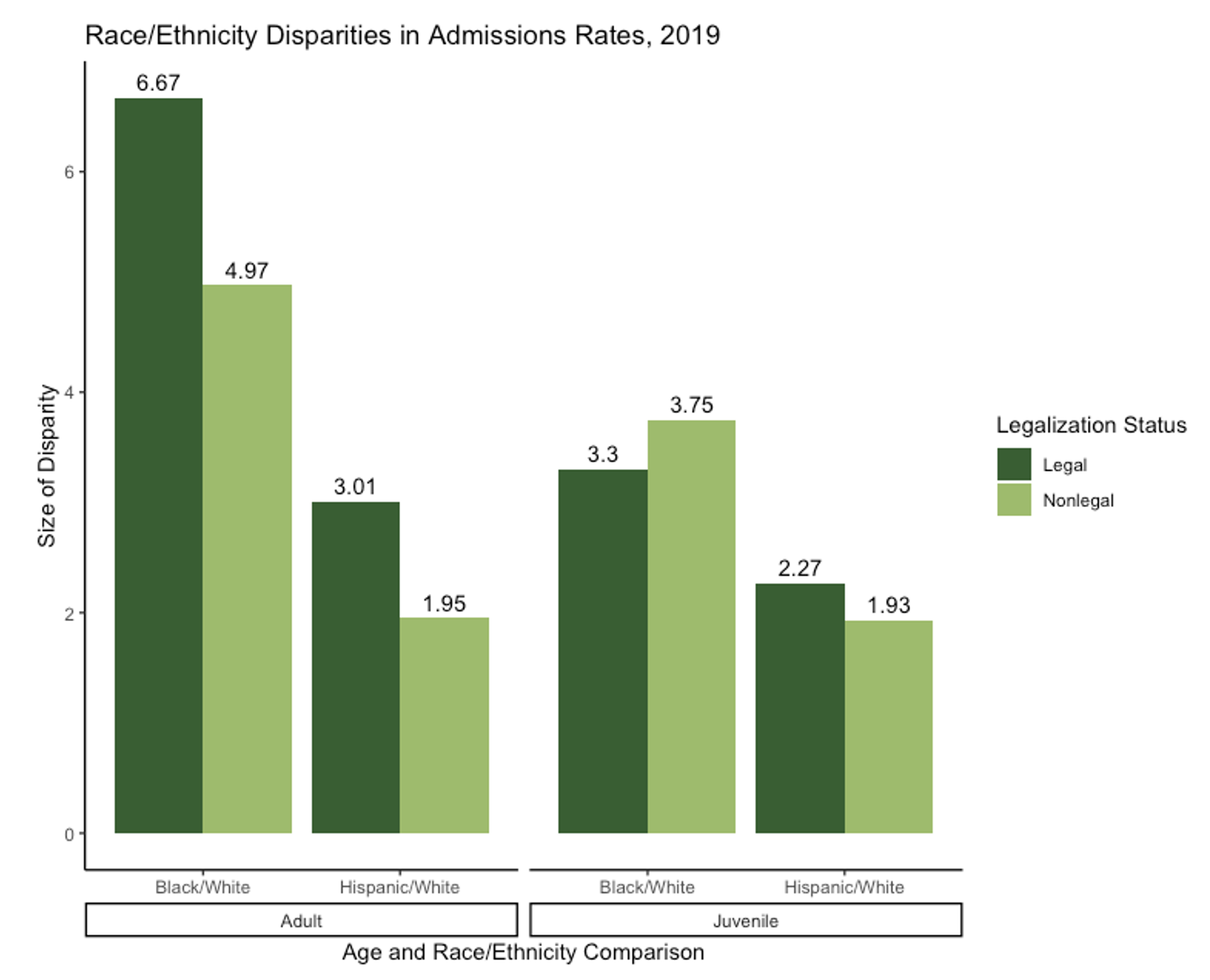
Note: A key highlight is that in 2019, Black adults in RCL states were admitted to treatment at a rate 6.67 times higher than white adults.
Implications
We observed a long-term decline in legally mandated cannabis treatment admissions in all states for all populations of study. However, recreational cannabis legalization was not statistically associated with these declines in treatment admissions when controlling for sociodemographic variables. This suggests that legalization does not necessarily alter how the legal system responds to cannabis use among individuals who interact with it. The significance of our control variables in various models — socioeconomic disadvantage, uninsured rates, government ideology — points to the potential for political, economic, and health factors to shape legal system outcomes.
While treatment admissions rates for juveniles declined more sharply than rates for their adult counterparts, adolescents were still referred and admitted to treatment at higher rates after reform. This is not surprising given that all RCL states restrict cannabis use and sales to individuals aged 21 and older. Still, adolescents use cannabis at lower rates than adults, suggesting that other factors contribute to the higher rates of legally mandated treatment admissions for this population, including the existence of additional pathways, like schools, through which juveniles encounter the legal system.[21]
White adults and juveniles experienced steeper declines in admissions rates than Black and Hispanic adults and juveniles. As a result, racial and ethnic disparities in admissions rates grew in both legal and nonlegal states, with a larger increase in legal states. This finding is consistent with prior research demonstrating that racial disparities in cannabis arrests tend to increase after legalization, even as the total number of cannabis arrests declines.[22]
Racial disparities in cannabis enforcement are systemic in the way they endure significant policy reform and manifest at multiple points along the legal system continuum. Black and Hispanic individuals are still more likely to encounter the police and be arrested and charged with cannabis-related offenses post-reform. When arrested and charged with non-cannabis offenses, Black and Hispanic defendants may be more frequently required to participate in legally mandated drug treatment as a condition of probation or deferred adjudication.
To be sure, there are cases in which legally-mandated cannabis treatment is appropriate, such as incidents of impaired driving that directly endanger others. We also do not dismiss the seriousness of cannabis use disorders (CUD), which evidence suggests are on the rise following legalization and increased access to high-potency THC products.[23] Like those with other substance use disorders, a small fraction of people with CUD receive treatment.[24] Unmet treatment needs stem largely from a dearth of effective and affordable care options, and this treatment shortage more severely affects disadvantaged groups, including legal system-involved individuals. [25] Recent evidence of an association between RCL and declines in voluntary cannabis treatment admissions further suggest that legalization could exacerbate the underutilization of treatment for CUD, perhaps by minimizing perceptions of CUD as a serious problem.[26]
Taken together, these trends may lead some to regard the continuation of legally mandated treatment for cannabis use in RCL states as a reasonable effort to connect disadvantaged populations with needed resources. However, the legal system’s efficacy in the treatment process is too limited and its adverse impacts are too severe to justify using it for this purpose.[27] The potential for legal consequences to follow the unsuccessful completion of treatment makes individuals vulnerable to the harms of legal system involvement, from reduced employment prospects to negative health outcomes. Black, Hispanic, and youth populations are more frequently subject to mandated drug treatment and thus are especially at risk of experiencing these harms. The problematic nature of this arrangement is enhanced when it occurs alongside a commercial cannabis industry that profits from greater levels of cannabis use.
Recommendations
Our study suggests that RCL has not fundamentally altered the legal system’s practice of requiring defendants who use cannabis to receive drug treatment, nor has it reduced racial and ethnic disparities in referral practices. These findings, coupled with prior research on legalization and cannabis arrest trends as well as evidence of disparate opportunities in nascent cannabis markets, suggest that Black, Hispanic, and youth populations are less likely to benefit from cannabis reform.
Based on our findings and the research to date, we recommend the following:
- Enact cannabis reform policies that explicitly target legal system features beyond arrest and prosecution.
- State lawmakers have begun to recognize the need to address other legal components of cannabis prohibition, as seen in the increased uptake of simplified or automatic record expungement policies for cannabis offenses that occurred prior to legalization.[28]
- To reduce unnecessary drug treatment requirements, policymakers should establish statutory provisions requiring clear evidence of a relationship between an individual’s cannabis use and the offense in question for probation departments and courtroom actors to mandate treatment participation.
- Minors who violate low-level cannabis laws and who are diagnosed with a cannabis use disorder may be referred to treatment, but oversight in such cases should be transferred from the legal system to community providers or other nonlegal system entities.
- Adopt education reforms that reduce school systems’ reliance on punitive disciplinary measures to respond to students’ use of alcohol and other drugs.
- Many school districts use alternative education settings for students engaged in alcohol- and other drug-related misconduct. Alternative schools have higher dropout rates than standard schools and some are overseen by juvenile probation departments. Alternative school placements increase the likelihood of legal involvement.[29]
- Minority students and Black students in particular are disproportionately placed in alternative education settings for nonviolent misconduct.
- While some states are implementing reforms aimed at ending the “school-to-prison pipeline,” many continue to take an overly punitive approach to substance use.[30]
- Interventions for adolescent substance use must take place outside of a disciplinary environment and must be attached to comprehensive service offerings that address student mental health, home environments, and other issues that may have led to substance use.
- Implement regulatory policies that discourage heavy consumption of high-potency THC products to reduce the prevalence of cannabis use disorders in RCL states.
- Heavy use of high-potency THC products may increase the risk of cannabis use disorder.[31]
- States may discourage high-potency THC consumption by capping the amount of THC allowed in products or assigning higher tax rates to products containing more THC.[32]
- State and local jurisdictions may also consider limiting the number of cannabis dispensary locations, as dispensary density is associated with heavier cannabis use among young adults.[33]
- Public health messaging aimed at cannabis users should provide accurate information and encourage realistic behavioral modifications for using more safely (e.g., taking “tolerance breaks”).[34]
- Federal leadership via regulating and monitoring the use and sale of cannabis products could significantly aid states in addressing the risks of greater prevalence of cannabis use disorders.[35]
- Invest resources for addressing substance use, like opioid settlement funds, into school- and community-based initiatives rather than law enforcement programs.
- Many states are in the process of determining how to allocate funds from large settlement agreements with pharmaceutical companies and drug distributors for their contributory role in the overdose crisis.
- Strategies to prioritize include overdose prevention, harm reduction, and school- and community-based prevention, treatment, and social assistance programs.
- Resources for substance use-related services should not be diverted to law enforcement. Police and legal system initiatives, such as enhanced drug enforcement efforts and drug courts, can be supported with already-existing public safety revenue streams.
Study Limitations
-
The TEDS-A data set relies on the quality of individual state reporting, which is highly variable. TEDS-A only captures publicly funded treatment admissions.
-
TEDS-A does not include data on offenses that triggered legal system treatment referrals, and our state-level analysis was not able to control for factors relating to the discretion of legal system actors to mandate individuals to cannabis use treatment. Future research should examine the relationship between offense and legal system referral practices surrounding cannabis use in legal states.
- State-level analyses do not account for local policy change; for example, in some nonlegal states the most populous jurisdictions have implemented de facto decriminalization policies that could affect state-level treatment referral trends.
Acknowledgments
We thank Zachre Andrews, Puneetha Goli, Yea Won Lee, Wendy Olivares, and Bianca Schutz, undergraduate students at Rice University, for their assistance with data collection, organization, and presentation.
Notes
[1] Substance Abuse and Mental Health Services Administration (SAMHSA), Treatment Episode Data Set (TEDS) 2019: Admissions to and Discharges From Publicly Funded Substance Use Treatment, Center for Behavioral Health Statistics and Quality (Rockville, MD: Substance Abuse and Mental Health Services Administration, 2021), https://www.samhsa.gov/data/sites/default/files/reports/rpt35314/2019_TEDS_3-1-22.pdf.
[2] This report is adapted from Katharine Neill Harris and Christopher F. Kulesza, “Exploring the Impact of Adult-Use Cannabis Legalization on Legal-System Referrals to Treatment for Cannabis Use: Do Age and Race Have a Moderating Effect?” Clinical Therapeutics 11, no. 39 (2023), https://doi.org/10.1016/j.clinthera.2023.03.006.
[3] David DeMatteo et al., “Outcome Trajectories in Drug Court: Do All Participants Have Drug Problems?” Criminal Justice Behaviors 36, no. 4 (2009): 354–68, https://doi.org/10.1177/0093854809331547; Noa Krawczyk et al., “Only One In Twenty Justice-Referred Adults In Specialty Treatment For Opioid Use Receive Methadone Or Buprenorphine,” Health Affairs 36, no. 12 (December 2017): 2046–53, https://doi.org/10.1377/hlthaff.2017.0890.
[4] MJ Biz Daily, “Where Marijuana is Legal in the United States,” updated November 13, 2023, https://mjbizdaily.com/map-of-us-marijuana-legalization-by-state/.
[5] DeMatteo et al. “Outcome Trajectories in Drug Court”; Ethan Sahker et al., “Efficacy of Brief Intervention for Drug Misuse in Primary Care Facilities: Systematic Review and Meta-Analysis Protocol,” BMJ Open 10, no. 9 (2020): e036633, http://dx.doi.org/10.1136/bmjopen-2019-036633; and Karen McElrath, Angela Taylor, and Kimberly K. Tran, “Black-White Disparities in Criminal Justice Referrals to Treatment: Addressing Treatment Need or Expanding the Diagnostic Net?” Behavioral Sciences 6, no. 21 (2016): 1–15, https://doi.org/10.3390/bs6040021.
[6] Krawczyk et al., “Only One In Twenty Justice-Referred Adults In Specialty Treatment”; Neill Harris and Jay Jenkins, “Diverted Opportunities: Gaps in Drug Treatment for Justice System-Involved Populations in Harris County, Texas” (Houston: Rice University’s Baker Institute for Public Policy, December 10, 2019), https://doi.org/10.25613/XZJH-GX92.
[7] Neill Harris and Kulesza, “Exploring the Impact of Adult-Use Cannabis Legalization on Legal-System Referrals to Treatment for Cannabis Use.”
[8] Bureau of Justice Statistics, “Law Enforcement,” 2021, https://bjs.ojp.gov/drugs-and-crime-facts/enforcement#arrests.
[9] Lindsay R. Standeven et al., “Trends in Cannabis Treatment Admissions in Adolescent/Young Adults: Analysis of TEDS-A 1992 to 2016,” Journal of Addiction Medicine 14, no. 4 (July/August 2020): 29–36, https://doi.org/10.1097/ADM.0000000000000586.
[10] COVID-19 impacted treatment admissions and survey collection, making data for 2020 incomparable to other years. That said, while the 2020 TEDS data reports substantial decreases in treatment admissions for all substances, the percentage of cannabis admissions originating with the legal system and the overrepresentation of Black and Hispanic/Latino populations in cannabis admissions remains relatively constant compared to 2019 (SAMHSA, Treatment Episode Data Set [TEDS] 2019).
[11] Approximately 13.6% of the U.S. population is Black. Black individuals comprised 20% of total treatment admissions in 2019, meaning they are especially overrepresented in cannabis treatment admissions. Hispanic/Latino individuals account for 19.1% of the U.S. population and made up 19% of cannabis treatment admissions and 14.5% of total treatment admissions in 2019 (SAMHSA, “2021 NSDUH: Detailed Tables,” January 4, 2023, https://www.samhsa.gov/data/report/2021-nsduh-detailed-tables).
[12] Mike Males and Lizzie Buchen, “Reforming Marijuana Laws: Which Approach Best Reduces the Harms of Criminalization? A Five-State Analysis,” Center on Juvenile and Criminal Justice, September 2014, http://www.cjcj.org/uploads/cjcj/documents/cjcj_marijuana_reform_comparison.pdf; Andrew D. Plunk et al., “Youth and Adult Arrests for Cannabis Possession After Decriminalization and Legalization of Cannabis,” JAMA Pediatrics 173, no. 8 (2019): 763, https://doi.org/10.1001/jamapediatrics.2019.1539; and Mary K. Stohr et al., “Effects of Marijuana Legalization on Law Enforcement and Crime,” National Criminal Justice Reference Service, July 2020, https://www.ojp.gov/pdffiles1/nij/grants/255060.pdf.
[13] Plunk et al., “Youth and Adult Arrests for Cannabis Possession.”
[14] Caislin L. Firth et al., “Did Marijuana Legalization in Washington State Reduce Racial Disparities in Adult Marijuana Arrests?” Substance Use & Misuse 54, no. 9 (May 2019): 1582–7, https://doi.org/10.1080/10826084.2019.1593007; Firth et al., “Implications of Cannabis Legalization on Juvenile Justice Outcomes and Racial Disparities,” American Journal of Preventive Medicine 58, no. 4 (February 2020): 562–9, https://doi.org/10.1016/j.amepre.2019.11.019; Nguyen K. Tran et al., “The Heterogenous Effect of Marijuana Decriminalization Policy on Arrest Rates in Philadelphia, Pennsylvania, 2009–2018,” Drug and Alcohol Dependence 212 (July 1, 2020): 1–8, https://doi.org/10.1016/j.drugalcdep.2020.108058; American Civil Liberties Union, A Tale of Two Countries: Racially Targeted Arrests in the Era of Marijuana Reform, 2020, https://www.aclu.org/report/tale-two-countries-racially-targeted-arrests-era-marijuana-reform; and Colorado Division of Criminal Justice, Impacts of Marijuana Legalization in Colorado: A Report Pursuant to C.R.S. 24-33.4-516, July 2021, https://cdpsdocs.state.co.us/ors/docs/reports/2021-SB13-283_Rpt.pdf.
[15] Brynn E. Sheehan, Richard A. Grucza, and Plunk, “Association of Racial Disparity of Cannabis Possession Arrests Among Adults and Youths With Statewide Cannabis Decriminalization and Legalization,” JAMA Health Forum 2, no. 10 (October 29, 2021): e213435, https://doi.org/10.1001/jamahealthforum.2021.3435.
[16] Neill Harris and Kulesza, “Exploring the Impact of Adult-Use Cannabis Legalization on Legal-System Referrals to Treatment for Cannabis Use.”
[17] Neill Harris and Kulesza, “Exploring the Impact of Adult-Use Cannabis Legalization on Legal-System Referrals to Treatment for Cannabis Use.”
[18] Data sources for control variables include TEDS-A; the U.S. Census American Community Survey; the Kaiser Family Foundation; and Department of Justice, Bureau of Justice Statistics. Government ideology measure from William D. Berry et al., “Measuring Citizen and Government Ideology in the American States, 1960-93,” American Journal of Political Science 42, no. 1 (1998): 327–48, https://doi.org/10.2307/2991759. Socioeconomic disadvantage measure adapted from Catherine E. Ross and John Mirowsky, “Neighborhood Disadvantage, Disorder, and Health,” Journal of Health and Social Behavior 42, no. 3 (2001): 258–76, https://doi.org/10.2307/3090214.
[19] Difference-in-difference analysis is a statistical technique used to determine whether a policy change has had an expected impact. This is achieved by comparing a group that experienced the policy change with a group that did not, both before and after the policy change. Difference-in-difference is “staggered” when the policy change in question occurs at different times in different places. For instance, in our analysis here, RCL states implemented the policy change in various years.
[20] Neill Harris and Kulesza, “Exploring the Impact of Adult-Use Cannabis Legalization on Legal-System Referrals to Treatment for Cannabis Use.”
[21] SAMHSA, “2021 NSDUH: Detailed Tables.”
[22] Sheehan, Grucza, and Plunk, “Association of Racial Disparity of Cannabis Possession Arrests”; Firth et al., “Did Marijuana Legalization in Washington State Reduce Racial Disparities in Adult Marijuana Arrests?”
[23] Magdalena Cerdá et al., “Association Between Recreational Marijuana Legalization in the United States and Changes in Marijuana Use and Cannabis Use Disorder from 2008 to 2016,” JAMA Psychiatry 77, no. 2 (November 13, 2019): 165–71, https://doi.org/10.1001/jamapsychiatry.2019.3254.
[24] SAMHSA, “2021 NSDUH: Detailed Tables.”
[25] Tawandra L. Rowell-Cunsolo and Meghan Bellerose, “Utilization of Substance Use Treatment Among Criminal Justice-Involved Individuals in the United States,” Journal of Substance Abuse Treatment 125 (June 2021):108423, doi:10.1016/j.jsat.2021.108423.
[26] Jeremy Mennis et al., “Recreational Cannabis Legalization Alters Associations Among Cannabis Use, Perception of Risk, and Cannabis Use Disorder Treatment for Adolescents and Young Adults,” Addictive Behaviors 138 (November 2022): https://doi.org/10.1016/j.addbeh.2022.107552.
[27] DeMatteo et al. “Outcome Trajectories in Drug Court”; Krawczyk et al., “Only One In Twenty Justice-Referred Adults In Specialty Treatment”; and Harris and Jenkins, “Diverted Opportunities: Gaps in Drug Treatment.”
[28] Blair Lozier, Valerie Newberg, and Dakota Thomas, “State Approaches to Marijuana Policy,” The Council of State Governments, February 13, 2023, https://www.csg.org/2023/02/13/state-approaches-to-marijuana-policy/.
[29] Deborah Fowler et al., “Texas’ School-to-Prison Pipeline: Ticketing, Arrest, and Use of Force in Schools,” Texas Appleseed, December 2010, https://www.njjn.org/uploads/digital-library/Texas-School-Prison-Pipeline_Ticketing_Booklet_Texas-Appleseed_Dec2010.pdf.
[30] For example, Texas recently passed a law that requires students caught vaping to be sent to a Disciplinary Alternative Education Program.
[31] Kat Petrilli et al., “Association of Cannabis Potency with Mental Ill Health and Addiction: A Systematic Review,” The Lancet Psychiatry 9, no. 9 (September 2022): 736–50, https://doi.org/10.1016/S2215-0366(22)00161-4.
[32] Rosalie Liccardo Pacula et al., “Federal Regulations of Cannabis for Public Health in the United States,” USC Schaeffer Center White Paper Series (July 18, 2022), https://healthpolicy.usc.edu/research/federal-regulations-of-cannabis-for-public-health-in-the-u-s/.
[33] Eric R. Pedersen et al., “Examining Associations Between Licensed and Unlicensed Outlet Density and Cannabis Outcomes from Preopening to Postopening of Recreational Cannabis Outlets,” The American Journal on Addictions 30, no. 2 (December 30, 2020): 122-30, https://doi.org/10.1111/ajad.13132.
[34] Days- or weeks-long breaks from cannabis use decrease a person’s tolerance; when they resume use they can consume less to achieve desired effects. For a tolerance break guide, see The University of Vermont Center for Health & Wellbeing, “T-Break: Take a Cannabis Tolerance Break,” https://www.uvm.edu/health/t-break-take-cannabis-tolerance-break.
[35] Liccardo Pacula et al., “Federal Regulations of Cannabis for Public Health.”
Appendix
Appendix Table 1 — State-Level Variables, Descriptive Statistics
Appendix Table 2 — Individual Level Descriptive Statistics, TEDS-A Data
Appendix Table 3 — Difference-in-Difference Results
Appendix Table 4 — Event Panel Analysis Results
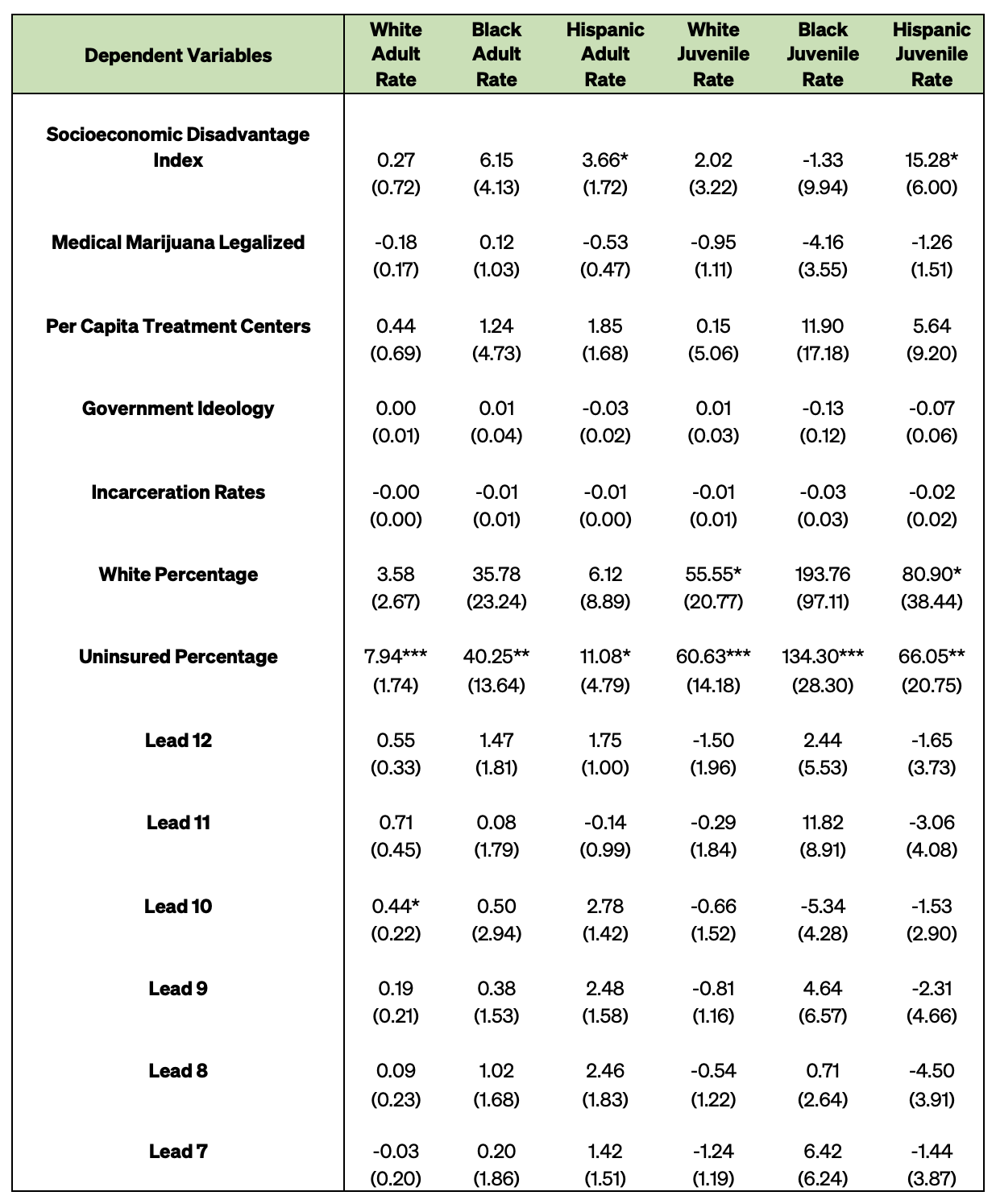
Appendix Table 4 — Event Panel Analysis Results Continued
Appendix Figure 1 — Results of Event Analysis
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


