
Key Takeaways
- The U.S. health care sector is grappling with a severe labor shortage, worsened by the long-term effects of the COVID-19 pandemic and an aging population, leading to widespread consequences, including increased patient rejection rates and overall strain on the system.
- Immigrants have historically been crucial in addressing health care labor shortages in the U.S., constituting a significant portion of the workforce in the sector, with the added benefit that migrant workers are often willing to work in high-demand and underserved areas.
- Restrictive and complex immigration policies are making it difficult for migrant workers to access health-related jobs and for the sector to meet a growing demand for care.
- Proposed immigration policy reforms include raising visa caps for health care workers, creating new health care-specific visa categories, reducing administrative burdens, and reforming occupational licensing laws to allow qualified immigrants to practice within their full scope of training.
- This report recommends developing federal and state programs to actively recruit health care workers from abroad, offering qualifying courses for migrants willing to work in the U.S., making flexible licensing requirements, and offering incentives such as expedited permanent residency and family reunification options for those willing to work in underserved areas.
Introduction
The U.S. health care sector is grappling with a severe labor shortage exacerbated by the COVID-19 pandemic and demographic changes, including a rapidly aging population.[1] While there was a recovery in the U.S. labor market after the COVID-19 pandemic, health care employment remained below pre-pandemic levels until recently, creating a critical gap in workforce supply.[2] Despite the recovery and the return to trend employment, shortages persist — demand for health care workers continues to outpace supply.[3]
Immigration has historically played a significant role in addressing health care labor shortages — with the added benefit that immigrants are often willing to work in underserved and low-income areas. Current policies, however, limit the potential contribution that immigrants can make in addressing health care workforce demands. Reforming immigration policies and creating specific paths for the health care sector could be a strategic solution to alleviate the current crisis. This report outlines the scope of the health care labor shortage, examines the role of immigrant workers, and proposes solutions focusing on comprehensive immigration reforms to support the health care sector.
To examine this issue, the Baker Institute Center for the U.S. and Mexico and the Institute for Humane Studies organized a one-day workshop in Washington, D.C., bringing together a diverse group of academics, policymakers, and industry professionals. This event focused on the workforce challenges facing the health care sector, the contributions of immigrant health care workers, and the role that key changes to the immigration and licensing system could play to alleviate these workforce shortages.
State of the Health Care Industry
The health care sector has experienced substantial job losses since March 2020, when the impact of the COVID-19 pandemic began to be felt. Despite a partial recovery, the sector still faces a significant deficit. In 2023, 13.8% of employed Americans worked in the health care and social assistance sector, a figure that has remained nearly constant since 2009. The pandemic temporarily disrupted this trend, causing a decline in 2021 and 2022, although it rebounded in 2023. However, compared to 2019 (the pre-pandemic level), this percentage has only grown by 0.3%, and it still has not fully recovered. When focusing solely on the health care sector, the findings are similar, as shown in Figure 1.
Figure 1 — Percentage of All US Nonfarm Employees Working in the Health Care Sector, 2000–23[4]

Note: Seasonally adjusted.
Assuming that the health care sector had continued to grow at pre-pandemic levels (using the average rate from 2009 to 2019), employment would have been 559,000 higher in 2023 for health care alone and 697,000 higher for health care and social assistance relative to their actual values. As illustrated in Figure 2, however, employment in the sector is still below its expected trend.
Figure 2 — Health Care Employment, 2000–23 (in thousands)
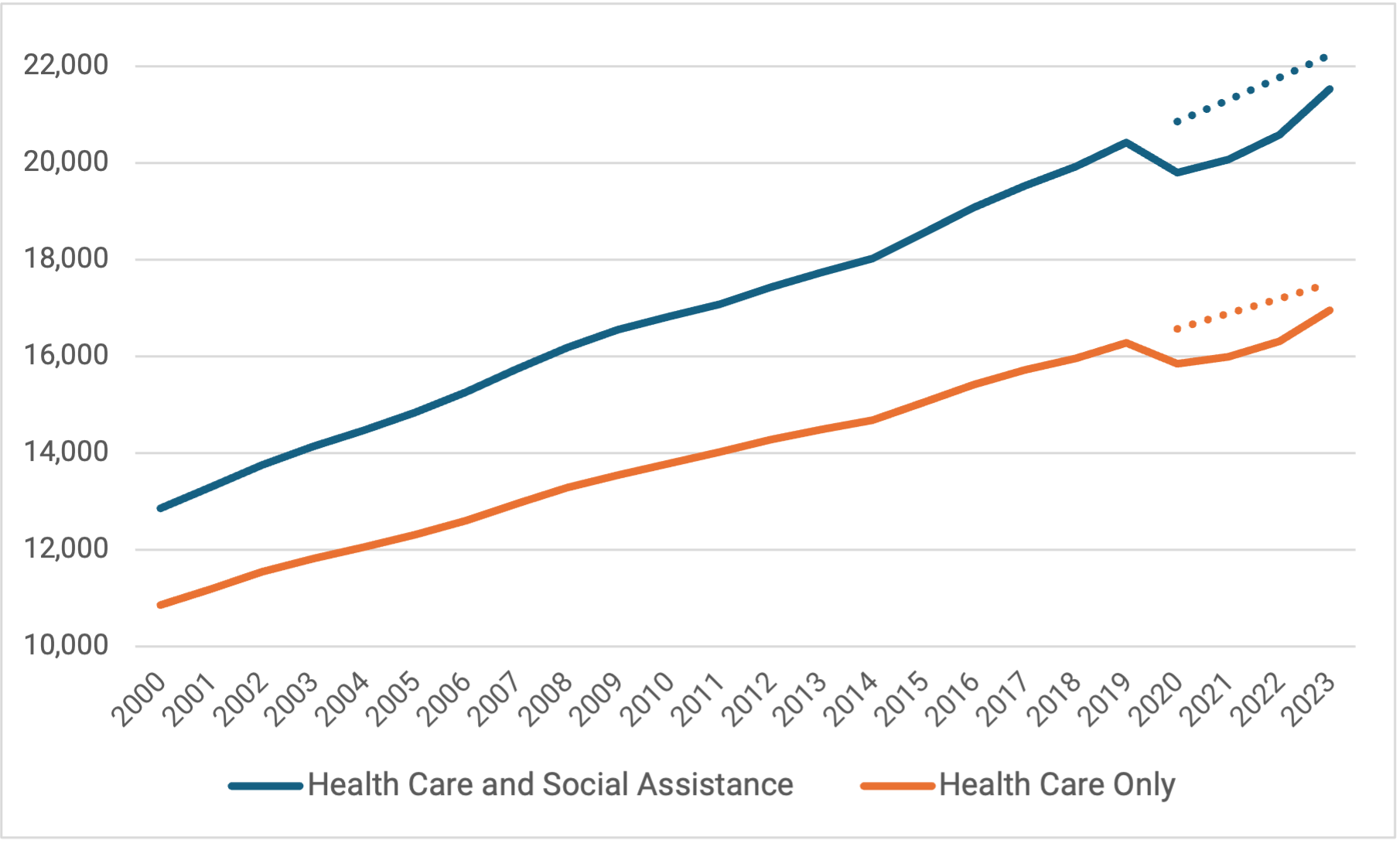
Note: Seasonally adjusted.
In the broader context of the health care workforce, both nurse and doctor shortages are projected:
- Physicians — Estimates range from a low of 38,000 to a high of 124,000 by 2034.[5]
- New primary care physicians — Projected shortfalls of between 20,200 and 40,400 by 2036.[6]
- Nurses — There are already acute shortages in states such as California, Texas, and New Jersey. California has an estimated shortfall of 44,500 registered nurses, and Texas has a projected shortfall of 15,900 registered nurses by 2030.[7]
Other health professions have also experienced shortages:
- Clinical laboratory specialists — In 2017, there were approximately 7.2% laboratory technician positions unfilled, and that figure could increase: BLS projects that this segment of the workforce will grow by 7% from 2023 to 2033 (around 214,700 new employees).[8]
- Dental sector — Approximately one-third of dental hygienists and administrative staff are retiring or will do so in five years or less.[9]
- Pharmacists and pharmacy specialists — Increased workloads on fewer people lead to shorter opening hours, longer wait times for medication and less patient counseling.[10] This issue may worsen due to an anticipated shortage of approximately 5,000 pharmacists over the next 15 years.[11]
Almost every state reports shortages in these roles, and this widespread issue impacts the health care system’s functioning and patients’ access to care. While technology is improving the productivity of workers, it is unlikely to replace the need for human-centered care. The emerging consensus is that the care sector will need to significantly expand its workforce across all categories to meet the growing demand.
Home Care Workers
Many home care providers are forced to reject patient admissions due to a severe staff shortage. In the home health care sector, which includes services provided by nurses and therapists, the referral-to-admission conversion rate was 55% in 2023, translating to 6.2 million patients without access to this service.[12] This results in hospitals facing significant logistical challenges when they cannot discharge patients into home care, leading to negative patient outcomes and increasing financial burdens on families. This intensifies pressures on family members, sometimes resulting in neglect or crisis situations. Currently, 14 million individuals of all ages receive home health care services annually. The industry generates $150–$160 billion a year, primarily funded by Medicaid, Medicare, Tricare, and the Older Americans Act of 1965, with minimal involvement from commercial payers.[13]
The home health care provider landscape includes nonprofit and for-profit organizations, both of which are facing a critical nurse shortage. Between 2020–21, the total supply of registered nurses decreased by over 100,000 — the largest drop in four decades.[14]
Compensation issues are a significant barrier: A workshop member reported making 160 job offers to nurses, all of whom declined due to insufficient pay.
- As the demand for home health care workers and aides increases, home health agencies cannot compete with hospitals on compensation since they primarily rely on reimbursement rates set by the Centers for Medicare and Medicaid Services (CMS) and Medicaid at the state level.
- Home care aides, the largest workforce segment, earn between $8.50 and $15 an hour, significantly lower than the average U.S. private sector wages of $32.26 in 2022 and $33.72 in 2023.[15]
- Medicaid and Medicare reimbursement rates are insufficient to adequately cover the recruitment of the frontline workforce at current market wages.
- Medicaid reimbursements vary considerably across the country, often putting nursing homes and home health agencies in high-demand labor markets at a competitive disadvantage compared to hospitals and other employment options.[16]
Although the home care subsector is not the only part of the industry affected by labor shortages, it reflects the broader challenges facing the sector today. As the U.S. experiences key demographic changes and rising demand for workers to care for an aging population, the labor market has become increasingly competitive.
Role of Immigrants in Health Care
To address labor shortages in the care industry, potential solutions include further investment in the domestic workforce and raising Medicaid and Medicare reimbursements for nursing homes to enable improved pay. However, many strategies focus on immigration, as it offers the quickest and most efficient way to gain workers in the sector:
- Reforming current visa programs to make them more efficient and less bureaucratic.
- Developing programs for migrants who are already trained health care workers to acquire U.S.-recognized qualifications.
- Revising occupational licensing laws to allow individuals to work to the full extent of their training.
- Creating new visas aimed at health care workers.
Immigrants and their children, already a vital part of the workforce, have driven over half of its growth over the past two decades.[17] In the health care sector, immigrants are 18.2% of all workers, including 26.5% of physicians and surgeons, 16% of registered nurses, and 23.1% of health care support staff.[18] Those numbers are significantly higher than the overall immigrant population rate in the U.S., which is approximately 14%. A recent Baker Institute report, using data from the American Community Survey, explores the increasing role of immigrants across various health care professions in the U.S., noting that immigrants are more likely to:
- Work in high-demand occupations, particularly in underserved areas and rural regions.
- Fill many frontline roles.[19]
Although the contribution of immigrants to the health care workforce varies considerably across the country, they are essential to the sector in nearly every state. This underscores their adaptability and highlights their crucial role in diverse settings, from urban centers to rural communities, demonstrating their integral part in maintaining and improving the U.S. health care system.
According to the Cato Institute, based on U.S. Census and American Community Survey data, approximately 34% of all health care workers in California are foreign-born.[20] Overall, the physician labor force contains a significant number of immigrants.[21] Even in states with generally low levels of immigration the proportion of foreign-born physicians and surgeons is relatively high; for example, 12% of physicians and surgeons in Arkansas are foreign-born.[22]
Despite this evidence and the clear need for qualified immigrants, current U.S. immigration policies are too restrictive to help the health care sector. The available pathways, often restrictive and complex, include:
- Temporary nonimmigrant visas — H-1B for highly skilled workers, J-1 for exchange visitors, TN visas under the United States-Mexico-Canada Agreement (USMCA), and O-1 visas for individuals with extraordinary abilities.
- Immigrant visa categories — EB-1 for non-U.S. citizens with extraordinary ability, outstanding professors and researchers, EB-2 for advanced degree holders, and those with national interest waivers.
Although during a pandemic-related recruiting drive, over 1,000 nurses arrived in the U.S. each month, the number of health care workers admitted under these visas is generally low.[23] Less than 4.7% of the 123,414 H-1B petitions approved for initial employment in fiscal year 2021 were for health care and medicine occupations.[24]
Several factors contribute to the bottleneck in health care worker immigration.
- Visa processing delays, long processing times, and administrative backlogs hinder timely availability of workers.
- Annual caps on visas, such as the H-1B, restrict the number of skilled professionals entering the U.S.
- Immigrant health care workers often face significant barriers in obtaining U.S. licenses.
- COVID-19 pandemic restrictions drastically reduced incoming health care workers, with lasting effects.
- Policies that restrict entry based on potential reliance on public assistance have deterred many qualified applicants.
Policy Recommendations
To alleviate the labor shortages in the health care workforce, this report recommends that the U.S. implements reforms in four specific policy areas:
- Immigration.
- Occupational licensing.
- Recruitment and retention.
- Immigration infrastructure investment.
1. Immigration Policy and Health Care Labor Supply
Several visa-related strategies should be implemented to streamline the entry of medical professionals.
- H-1B visas — Raising the annual cap for H-1B visas for health care workers (as has already been done for academia).
- New visa categories — Creating new sector-specific visa categories with expedited processing and reduced bureaucratic.
These two measures would significantly increase the pool of available workers, across a variety of medical specialties, from countries whose training is compatible with U.S. standards. Leveraging existing programs, such as the TN visa program, offers another way to address these shortages.[25]
- TN visa program expansion — This program enables easier work authorization in the U.S. for Canadian and Mexican workers for certain medical professions. Ensuring that the TN visa categories include occupations where the U.S. needs additional workers is an important step toward maximizing the potential of this visa. Additionally, increasing awareness and utilization of TN visas specifically for health care professionals from these countries, along with simplifying the application process for other visas, could provide a swift solution to workforce needs in this sector.
- New specialized visas — Another possibility is to introduce specialized visas for professions affected by shortages, prioritizing graduate students in fields related to the care. This approach would bypass many bureaucratic issues associated with standard visa processing and offer a skilled pathway for people to immigrate to the U.S.
By implementing strategies such as expanding and enhancing the TN visa program with more medical occupations, the United States will be able to take advantage of existing systems and geographical proximity to bolster its medical workforce quickly.
2. Occupational Licensing Reforms
As well as incentivizing U.S. institutions to train more health professionals, there are several ways to improve immigrants’ access to the sector.
- Enabling foreign-born workers to upskill — Introducing curricula for foreign-born workers to upskill to U.S. standards and reforming occupational licensing laws could rapidly alleviate health care worker shortages by allowing qualified immigrants to practice fully within their training scope.
- Reciprocal agreements — Establishing reciprocal agreements with countries known for their high-quality health care education, such as the Philippines and India, would enable recognition of foreign medical qualifications and make obtaining licensure easier in the U.S., enabling skilled professionals to enter the workforce more quickly.
- National licensing measures — Implementing a national licensing exam for foreign-trained health care professionals would standardize the certification process and reduce state variability. This move towards universal licensure could be complemented by domestic initiatives already underway in the United States.[26] Twenty-six states have implemented Universal Licensing Agreements for various professions, promoting mobility within the country.[27]
- Specialized compacts — Facilitating cross-state practice for advanced medical professionals, specialized compacts such as the Interstate Medical Licensure Compact (IMLC) for physicians and surgeons, the Advanced Practice Registered Nurses Compact (APRN Compact) for advanced practice registered nurses, and the Nurse Licensure Compact (NLC) for registered nurses are playing a vital role.[28]
These national efforts, combined with international reciprocal agreements, could significantly improve workforce mobility and help address labor shortages by allowing professionals to practice to the full extent of their training across different jurisdictions.
3. Recruitment and Retention Reforms
Developing federal and state programs to actively recruit health care workers from abroad is another way to address the issue. Such initiatives should focus on countries with high levels of health care training and offer attractive incentives, such as expedited permanent residency and family reunification options for those who commit to working in underserved areas. Several states are exploring programs like the International Medical Graduate (IMG) initiative, which allows unmatched physicians who graduated from medical schools outside the U.S. to practice fully in exchange for working in rural or underserved areas of the country.[29] Expanding these reforms beyond physicians has the potential to reduce shortages in other health care sectors as well.
By focusing on countries with robust health care education systems and offering clear pathways to residency and practice, these programs could attract highly qualified professionals to fill critical gaps in the U.S. system.
4. Reform and Invest in the Immigration Infrastructure
Two significant reforms could improve the immigration process, enabling an improved response to U.S. market forces.
- Reforming the public charge rule to exclude direct care health workers, such as frontline workers, would reduce the chance of entry denial based on potential use of public assistance.
- Developing the immigration infrastructure by increasing funding and resources for immigration processing would shorten lengthy processing periods, reduce delays, and ensure timely entry for health care workers. Administrative delays raise the transaction costs for migration and potentially discourage health care immigrants from coming to the U.S.
These reforms would incentivize migration from those who have previously been discouraged from applying by the public charge rule or the lengthy process.
Conclusion
The U.S. healthcare sector is facing a critical labor shortage that could undermine patient care and the overall functionality of the system. This shortage is particularly concerning given the large number of Americans with chronic conditions who require ongoing medical care, as well the country’s accelerating demographic shifts, including an aging population and a fast-retiring workforce. A lack of healthcare professionals can have far-reaching consequences, negatively impacting care quality and patient outcomes, increasing costs for private and public insurance programs — particularly relevant as both Medicare and Medicaid face increasing scrutiny due to rising health care costs.
Immigration reform targeted toward health care workers can be a crucial part of the strategy to meet the need. Existing immigration policies are too restrictive and reform should focus on several key areas:
- Expanding visa categories for health care workers.
- Increasing caps for existing visas.
- Streamlining licensing processes.
- Enhancing recruitment and retention efforts.
- Addressing policy barriers.
Implementing the comprehensive reforms recommended in this report would produce multiple benefits to the U.S. health care system. It would help to:
- Meet the country’s growing health care needs and the challenges of an aging population.
- Support economic growth by improving access to efficient health care.
- Maintain high-quality patient services while promoting greater access to care.
In addition, these reforms would create a more flexible and responsive health care workforce, better equipped to address shortages in underserved areas.
By adopting these recommendations, policymakers can strengthen the U.S. health care system, ensuring improved care for all Americans, and build a more resilient and efficient health care infrastructure for the future.
Acknowledgments
The workshop and this publication are generously supported by a grant from the Charles Koch Foundation and the Institute for Humane Studies.
Notes
[1] Steven Ross Johnson, “Staff Shortage Choking US Health Care System,” U.S. News, July 8, 2022, https://www.usnews.com/news/health-news/articles/2022-07-28/staff-shortages-choking-u-s-health-care-system.
[2] U.S. Bureau of Labor Statistics, “Employment Recovery Continues in 2021, with Some Industries Reaching or Exceeding Their Prepandemic Employment Levels,” May 2022, https://www.bls.gov/opub/mlr/2022/article/employment-recovery-continues-in-2021.htm; Imani Telesford et al., “What Are the Recent Trends in Health Sector Unemployment?,” Peterson-KFF Health System Tracker, https://www.healthsystemtracker.org/chart-collection/what-are-the-recent-trends-health-sector-employment/.
[3] American Hospital Association, “Workforce Shortages and Violence Are Rising Concerns in State of Nursing Poll,” accessed September 15, 2024, https://www.aha.org/aha-center-health-innovation-market-scan/2024-03-26-workforce-shortages-and-violence-are-rising-concerns-state-nursing-poll.
[4] “Nonfarm, commonly known as Total Nonfarm Payroll, is a measure of the number of U.S. workers in the economy that excludes proprietors, private household employees, unpaid volunteers, farm employees, and the unincorporated self-employed. This measure accounts for approximately 80% of the workers who contribute to gross domestic product (GDP).” See FRED, “All Employees, Total Nonfarm,” St. Louis Fed, updated November 1, 2024, https://fred.stlouisfed.org/series/PAYEMS.
[5] Association of American Medical Colleges (AAMC), “AAMC Report Reinforces Mounting Physician Shortage,” press release, June 11, 2021, https://www.aamc.org/news/press-releases/aamc-report-reinforces-mounting-physician-shortage.
[6] AAMC, “The Complexities of Physician Supply and Demand: Projections from 2021 to 2036,” March 2024, https://www.aamc.org/media/75236/download?attachment.
[7] Catherine Burger, “The States with the Largest Nursing Shortages,” RegisteredNursing.org, updated September 4, 2024, https://www.registerednursing.org/articles/largest-nursing-shortages/.
[8] Judy Stone, “We’re Facing A Critical Shortage of Medical Laboratory Professionals,” Forbes, April 28, 2022, https://www.forbes.com/sites/judystone/2022/04/28/were-facing-a-critical-shortage-of-medical-laboratory-professionals/; and US Bureau of Labor Statistics, “Employment Projections,” last modified August 29, 2024, https://www.bls.gov/emp/tables/occupational-projections-and-characteristics.htm.
[9] ADA Health Policy Institute, “Dental Workforce Shortages: Data to Navigate Today’s Labor Market,” https://www.ada.org/-/media/project/ada-organization/ada/ada-org/files/resources/research/hpi/dental_workforce_shortages_labor_market.pdf.
[10] John Voorhees, “The US Pharmacist Shortage,” Applied Policy, January 12, 2023, https://www.appliedpolicy.com/the-u-s-pharmacist-shortage/.
[11] Killian Meara, “Student, Staffing Shortages Continue to Impact Pharmacy Profession,” August 6, 2024, Drug Topics, https://www.drugtopics.com/view/student-staffing-shortages-continue-to-impact-pharmacy-profession.
[12] Homecare Homebase, “Leading Care Forward by Advocating for Our Customers and Their Patients,” comment letter, August 23, 2023, https://hchb.com/wp-content/uploads/2023/08/HCHB-CMS-CY24-Comment-Letter-1.pdf.
[13] National Association for Home Care and Hospice, “The Value of Home Care,” toolkit, March 18, 2018, https://www.nahc.org/wp-content/uploads/2018/03/18-MOW-Toolkit-Value.pdf; Centers for Medicare and Medicaid Services (CMS), “National Health Expenditure (NHE) Fact Sheet,” last modified September 10, 2024, https://www.cms.gov/data-research/statistics-trends-and-reports/national-health-expenditure-data/nhe-fact-sheet.
[14] Makinizi Hoover et al., “Data Deep Dive: A National Nursing Crisis,” US Chamber of Commerce, January 29, 2024, https://www.uschamber.com/workforce/nursing-workforce-data-center-a-national-nursing-crisis#:~:text=From%202020%20to%202021%2C%20the,in%20the%20last%20forty%20years.
[15] Federal Reserve Bank of St. Louis, “Average Hourly Earnings of All Employees: Total Private,” updated September 6, 2024, https://fred.stlouisfed.org/series/CES0500000003.
[16] Marc Joffe and Krit Chanwong, “Containing Medicaid Costs at the State Level,” Cato Institute, February 6, 2024, https://www.cato.org/policy-analysis/containing-medicaid-costs-state-level#medicaids-role-overall-us-health-system.
[17] Pia Orrenius and Chloe Smith, “Without Immigration, US Economy Will Struggle to Grow,” Federal Reserve of Dallas, April 9, 2020, https://www.dallasfed.org/research/economics/2020/0409.
[18] Jeanne Batalova, “Immigrant Health-Care Workers in the United States,” Migration Policy Institute, April 7, 2023, https://www.migrationpolicy.org/article/immigrant-health-care-workers-united-states.
[19] Shishir Shakya, “Understanding the Role of Immigrants in the US Health Sector: Employment Trends from 2007–21,” Rice University’s Baker Institute for Public Policy, January 3, 2024, https://doi.org/10.25613/JSF6-J097.
[20] Alex Nowrasteh and Michelangelo Landgrave, “Immigrant Health Care Workers by Occupation and State,” Cato Institute, May 13, 2020, https://www.cato.org/publications/publications/immigrant-health-care-workers-occupation-state#workers-occupation-nativity-state.
[21] American Immigration Council, “Foreign-Trained Doctors Are Critical to Serving Many US Communities,” January 2018, https://www.americanimmigrationcouncil.org/sites/default/files/research/foreign-trained_doctors_are_critical_to_serving_many_us_communities.pdf.
[22] Alex Nowrasteh and Michelangelo Landgrave, “Immigrant Health Care Workers by Occupation and State,” Cato Institute, May 13, 2020, https://www.cato.org/publications/publications/immigrant-health-care-workers-occupation-state#.
[23] Stephanie Nolen, “Rich Countries Lure Health Workers from Low-Income Nations to Fight Shortages,” New York Times, January 24, 2022, https://www.nytimes.com/2022/01/24/health/covid-health-worker-immigration.html.
[24] Department of Homeland Security and US Citizenship and Immigration Services, “Characteristics of H-1B Specialty Occupation Workers,” March 2, 2022, https://www.uscis.gov/sites/default/files/document/data/H1B_Characteristics_Congressional_Report_FY2021-3.2.22.pdf.
[25] Tony Payan and José Iván Rodríguez-Sánchez, “Revamping the TN Visa to Get Workers Where the US Needs Them,” Rice University’s Baker Institute for Public Policy, June 7, 2023, https://www.bakerinstitute.org/research/revamping-tn-visa-get-workers-where-us-needs-them#_ednref11.
[26] Goldwater Institute, “Breaking Down Barriers to Work with Universal Recognition: Frequently Asked Questions,” updated March 2022, https://www.goldwaterinstitute.org/universalrecognition/.
[27] Kihwan Bae and Darwyyn Deyo, “2024 Update to the Survey of Universal Licensing Reforms in the United States,” West Virginia University’s John Chambers College of Business and Economics, July 2024, https://csorwvu.com/policy-brief-survey-of-universal-licensing-reforms-in-the-united-states-2024/.
[28] “Interstate Medical Licensure Compact,” 2021, www.imlcc.org; “Advanced Practice Registered Nurses Compact,” 2024, https://www.aprncompact.com.; and “Nurse Licensure Compact,” National Council of State Boards of Nursing (NCSBN), 2024, https://www.nursecompact.com/.
[29] Jeffrey A. Singer, “More States Move to Let Experienced Foreign Doctors Serve Their Patients,” Cato Institute, March 14, 2024, https://www.cato.org/blog/more-states-move-let-experienced-foreign-doctors-serve-their-patients.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


