
Introduction
Health care professionals were widely praised for their work on the front lines of the COVID-19 pandemic. But the U.S. health care sector faces longstanding challenges that undermine its capacity to respond to future health threats and provide critical care. These challenges include an aging population, worker shortages, and the underrepresentation of minorities, a problem that has important implications for health care delivery. Meanwhile, policymakers have the difficult task of simultaneously expanding health care access, improving health care quality, and reducing costs without compromising compassionate care.
Immigrants and the U.S. immigration system offer a potential solution to the sector’s challenges. This report highlights various trends and statistics related to immigrant health care workers from 2007 to 2021, illustrating their critical role in the field. We also review various legal pathways for foreign medical professionals to enter the U.S. labor force and help address health worker shortages, including the J-1 Visa Exchange Visitor Program, the Conrad 30 Waiver Program, and innovative state and private sector programs.
Other publications have briefly analyzed the share of immigrant health care professionals working in the United States in specific years (Batalova 2023; Nowrasteh and Landgrave 2020). Our report is distinctive in that it showcases trends among various health care subindustries over a longer period of time, utilizing one-year estimates from public use microdata obtained though the U.S. Census Bureau’s American Community Survey (ACS).
National Trends, Numbers, and Shares of Immigrants
Total U.S. Population and Immigrants
We present trends in U.S. population growth and the percentage of immigrants in the U.S. population in Figures 1a and 1b. The native-born population included in our count encompasses individuals born in the United States, Puerto Rico, Guam, the U.S. Virgin Islands, and the Northern Marianas, as well as abroad to U.S. citizen parents. Our count of immigrants, or the U.S. foreign-born population, includes individuals who obtained U.S. citizenship through naturalization and non-U.S. citizens, such as legally admitted immigrants, refugees, undocumented immigrants, and temporary residents (e.g., students and temporary workers). These definitions of “native-born” and “foreign-born” are consistent with those used by the Bureau of Labor Statistics (BLS) and the ACS. (The BLS and ACS, however, do not use a unified definition of “immigrant.”)
Figure 1a — Total U.S. Population, 2007-2021
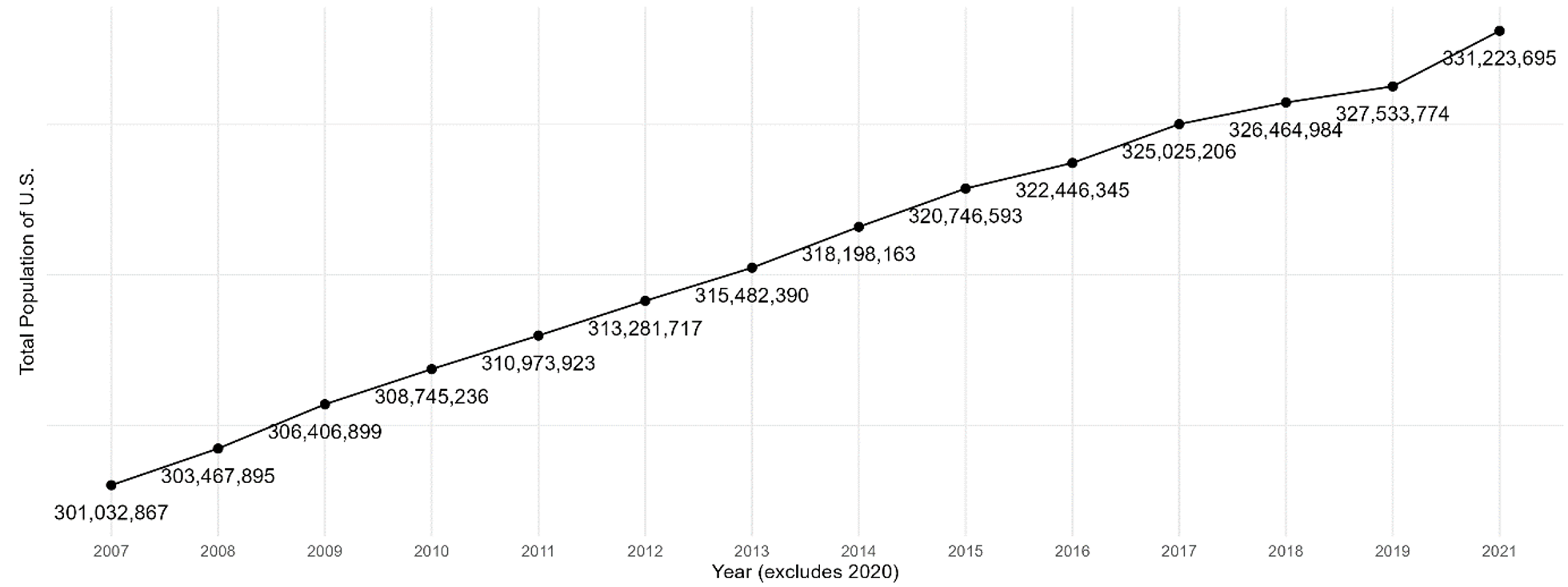
Figure 1b — Immigrant Share of Total U.S. Population, 2007-2021
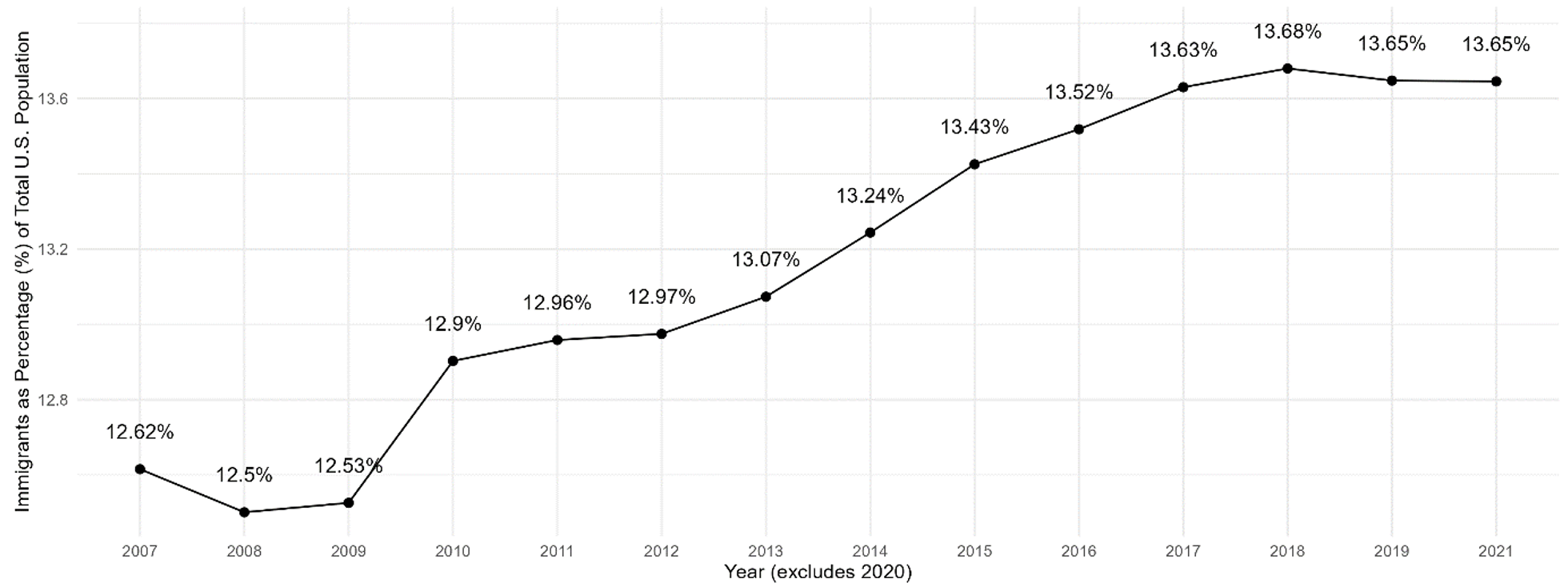
Figure 1b depicts the share or percentage of immigrants in the total U.S. population. As an illustration, the total population in 2021 amounted to 331.22 million, with immigrants comprising approximately 13.65%, or roughly 45.21 million individuals. According to the Pew Research Center, the share of immigrants in the total population is approaching a record high (Connor and Budiman 2019). The highest historical percentage of immigrants recorded among Americans was 14.8% in 1890.
The U.S. experienced substantial growth in its foreign-born population from the early to late 1800s, primarily consisting of Northern Europeans. However, in the early 1900s, a significant influx of new immigrants originated mainly from Italy, Poland, and other parts of Southern and Eastern Europe (Martin 2021). During the 1920s, new restrictive immigration laws resulted in a decline in the foreign-born population, a trend that persisted until the establishment of the Immigration and Nationality Act in 1965 (Connor and Budiman 2019).[1]
Total Number of U.S. Workers and Employed Immigrants
Figures 2a and 2b display the total number of working civilians in the U.S. aged 16 and over, along with the corresponding share of immigrants. This population includes employed, working civilians and civilians employed but temporarily absent from work at the time of survey data collection. The number of civilians working in the U.S. aged 16 and over excludes people who are unemployed, members of the U.S. armed forces, members of the U.S. armed forces temporarily absent from work at the time of survey data collection, and people who are not part of the labor force. From 2007 to 2018, the percentage of immigrants among workers aged 16 and above increased from 15.81% to 17.36%.
Figures 1a through 2b show a striking trend wherein immigrants are generally overrepresented in the labor market compared to their share in the total population. From 2007-2021, as the U.S. population grew from 301 million to 331 million, the immigrant share of the total population increased from 12.62% to 13.65%. Meanwhile, the percentage of immigrants among all workers aged 16 and above rose from 15.81% to 17.17%.
Figure 2a — Total Workers in the United States, 2007-2021
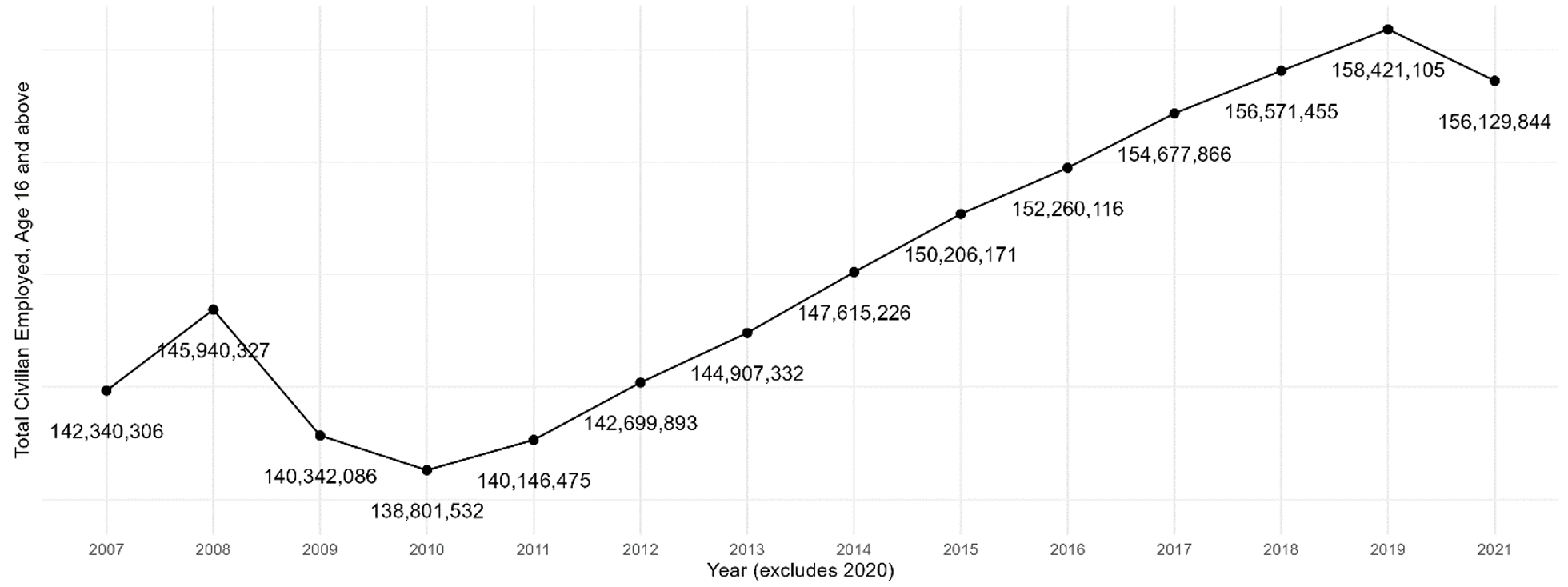
Note Includes workers aged 16 and over.
Figure 2b — Immigrant Share of U.S. Workers, 2007-2021
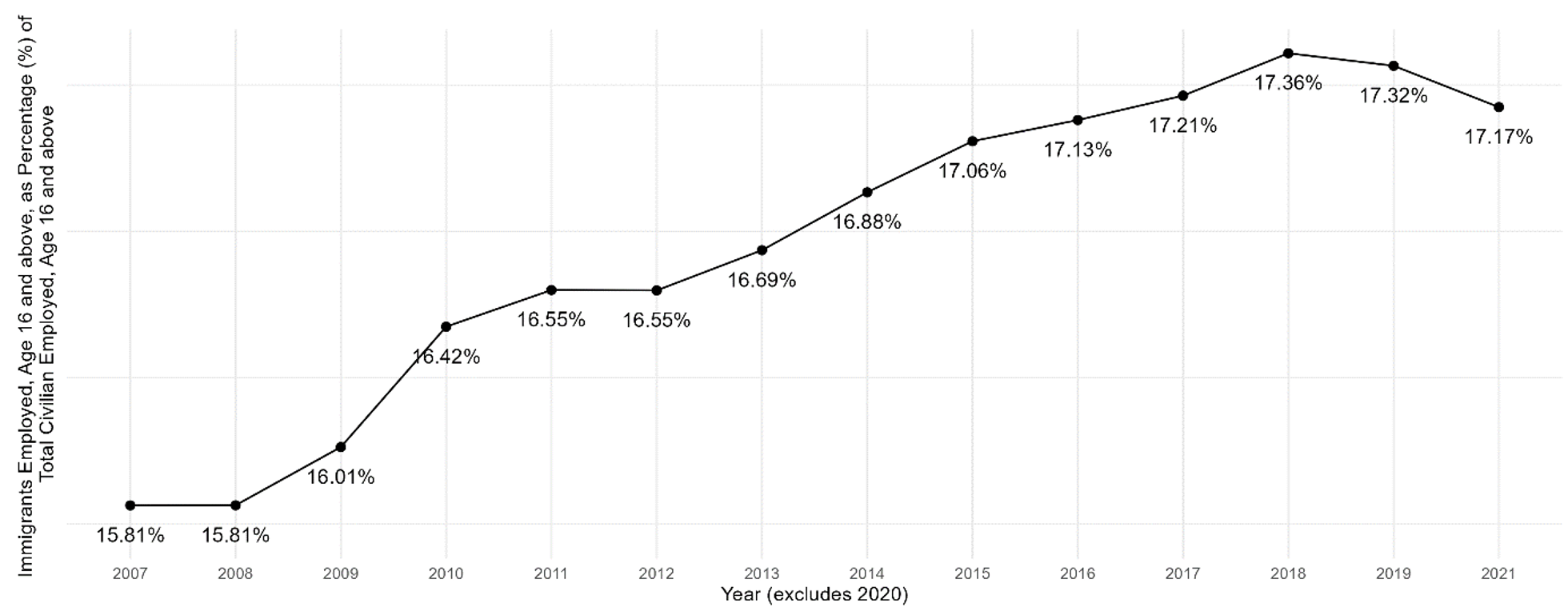
Note Includes workers aged 16 and over.
Health Care and Social Assistance Sector
The health care and social assistance sector includes establishments that provide medical care in hospitals, clinics, and doctor’s offices; nursing and residential care; and social assistance, such as family and child care services. Five out of the 20 industry groups projected to grow the fastest from 2019 to 2029 are in health care and social assistance, the fastest-growing sector of the economy.[2]
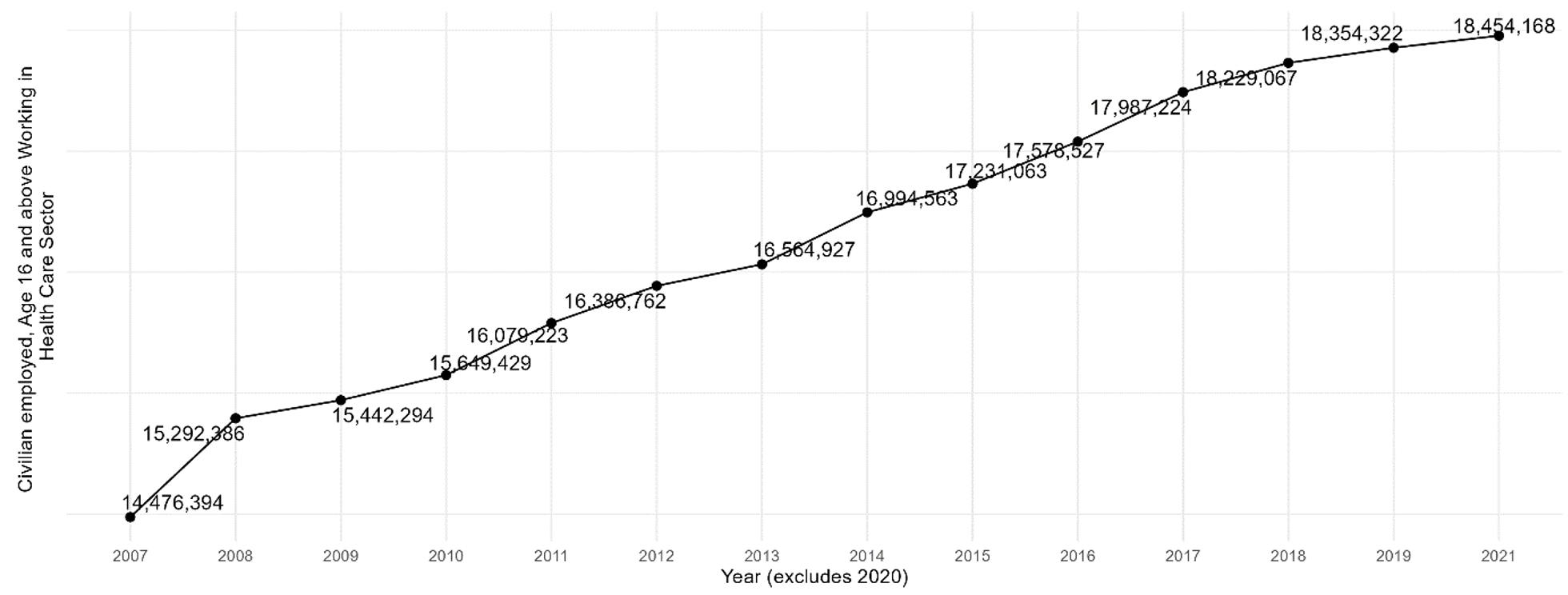
Figures 3a and 3b illustrate the number of U.S. health care workers and the immigrant share of the health care workforce from 2007 to 2021. During this period, the number of workers grew from 14.5 million to 18.5 million, and the proportion of immigrants working in health care increased from 14.22% to 16.52%.
Figure 3a — Total U.S. Health Care Sector Workers, 2007-2021
Note Includes workers aged 16 and over.
Figure 3b — Immigrant Share of U.S. Health Care Sector Workers, 2007-2021

Note Includes workers aged 16 and over.
The health care sector, as categorized by the North American Industry Classification System and the Bureau of Labor Statistics, comprises workers within various subsectors. (Appendix A provides a detailed presentation of trends within the U.S. health care sector, arranged in descending order of the subsectors’ respective shares.) The subsectors include: ambulatory health care services, including outpatient care centers and offices of physicians, dentists, optometrists, chiropractors, and other practitioners; hospitals, including general medical, surgical, specialty, psychiatric, and substance abuse hospitals; nursing and residential care facilities; and social assistance.
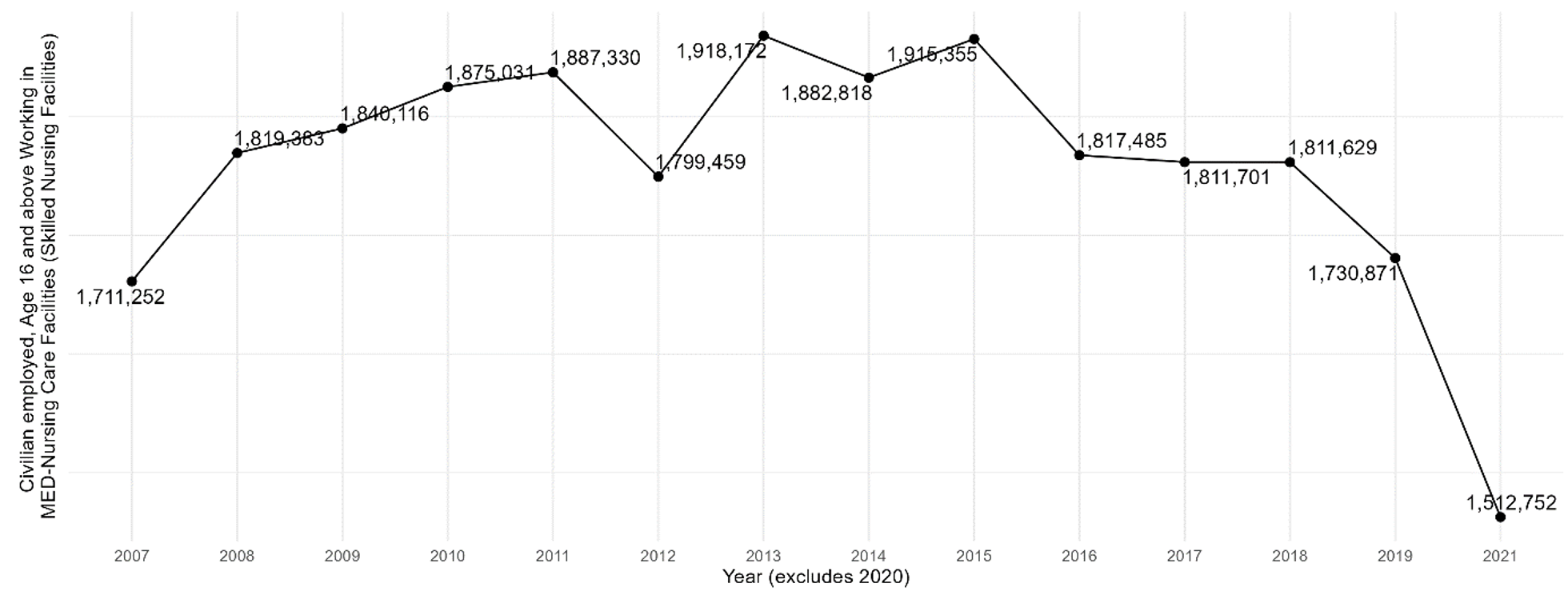
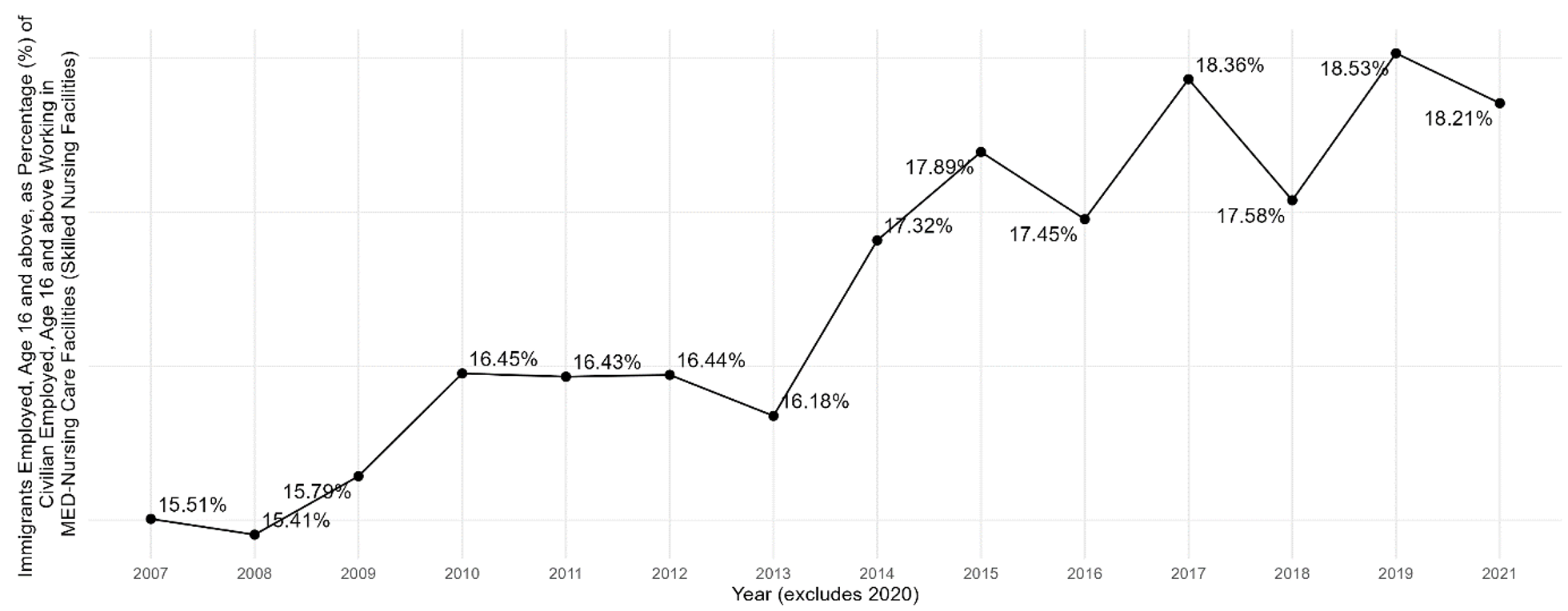
The nursing and residential care facilities subsector provides medical and nursing care for patients who require more than in-home care by trained medical professionals, such as nurses, therapists, and doctors, who are available around the clock. In addition, these facilities are used for short-term stays after hospitalization, surgery, or injury, with patients staying in skilled care facilities to heal and gain strength before returning home. Figure 4 shows that in nursing care facilities, the number of workers increased from 1.7 million in 2007, with an immigrant share of 15.51%, to a peak of 1.9 million in 2013, with an immigrant share of 16%. However, this trend in growth has declined; by 2021, there were 1.5 million workers in the subsector, with an immigrant share of nearly 18.21%.
Figure 4a — Total Workers in U.S. Nursing Care Facilities, 2007-2021
Note Includes workers aged 16 and over; excludes residential care facilities.
Figure 4b — Immigrant Share of Workers in U.S. Nursing Care Facilities, 2007-2021
Note Includes workers aged 16 and over; excludes residential care facilities.
Social Assistance
Another important part of the health services sector is the social assistance subsector, which includes establishments that provide social assistance services directly to individuals and families in need. These services include various activities such as child care, emergency relief, housing assistance, and vocational rehabilitation. The social assistance subsector includes some of the fastest-growing industries in the United States.
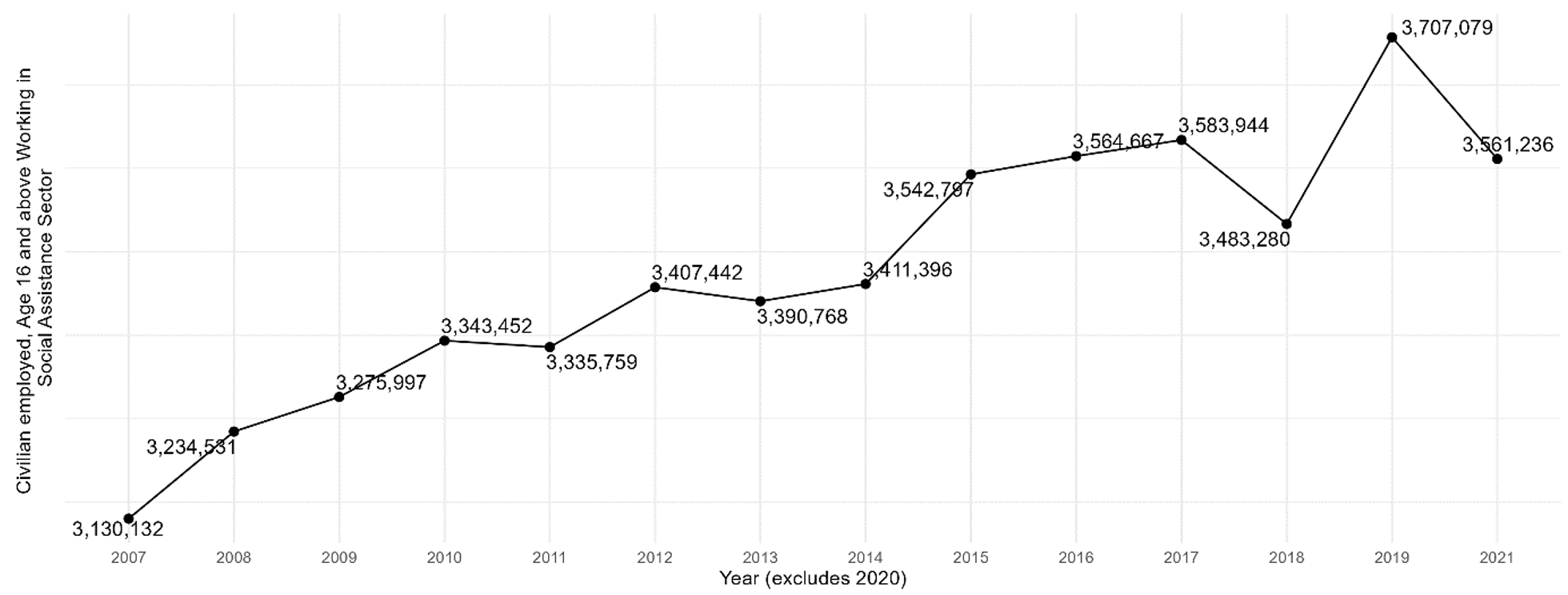
Figures 5a and 5b show the employment trend in the social assistance subsector and the immigrant share of the workforce. In 2007, 3.13 million people were employed, and immigrants made up 13.54% of the subsector’s workforce. In 2021, 3.56 million people were employed, with immigrants accounting for 17.8%.
Figure 5a — Total Workers in U.S. Social Assistance, 2007-2021
Note Includes workers aged 16 and over.
Figure 5b — Immigrant Share of Workers in U.S. Social Assistance, 2007-2021
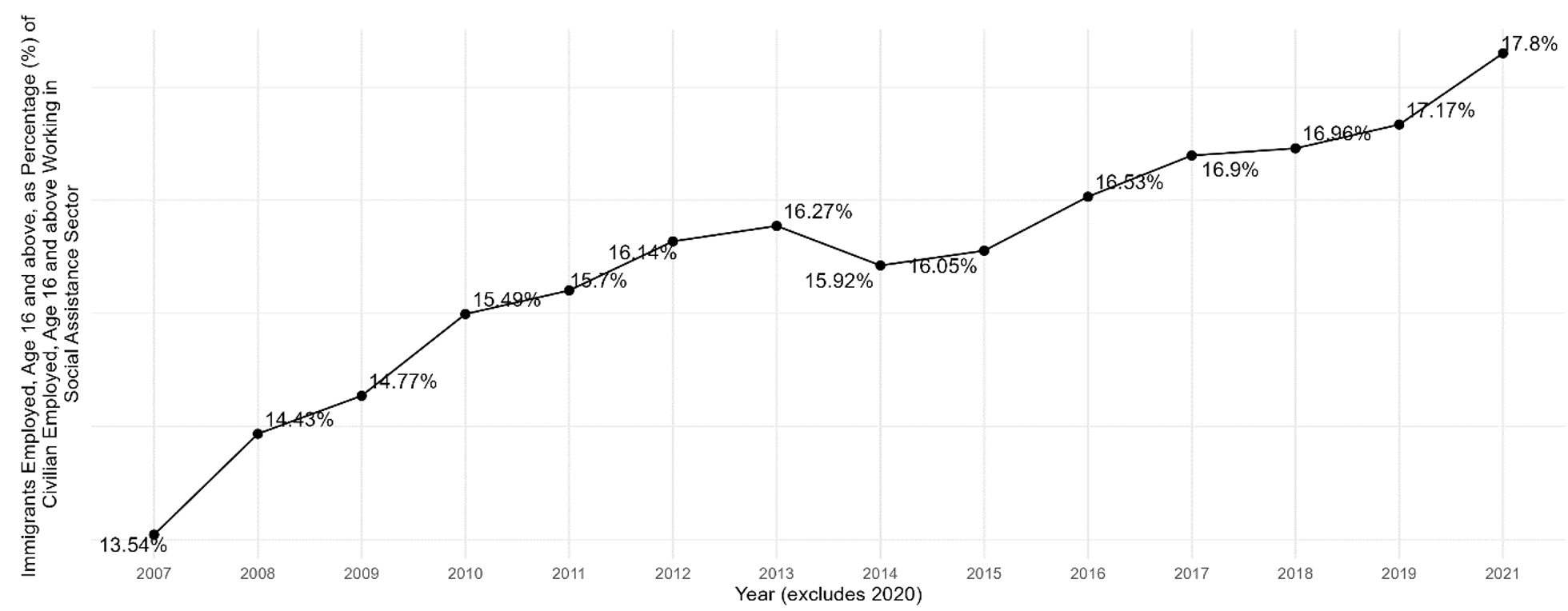
Note Includes workers aged 16 and over.
Like the health care sector, the social assistance subsector comprises workers within various industry groups. (In Appendix B, we present detailed trends within the U.S. social assistance subsector in descending order of industry group share.) These include individual and family services, child day care services, community food and housing and emergency and other relief services, and vocational rehabilitation services. The BLS projects that individual and family services are the fastest-growing industry group in the United States (see Appendix B, Figure B1). Meanwhile, the total number of workers in child day care and vocational rehabilitation services is declining, but their share of immigrant workers is rising (see Appendix B, Figures B2 and B4.).
Health Care Occupations
The health care field encompasses a range of roles and responsibilities, including health care technicians and practitioners such as registered nurses, physicians, surgeons, and licensed practical and licensed vocational nurses. Additionally, there are health care support occupations in the fields of nursing, psychiatry, home health, and medical assistance.[2]
Registered nurses, the largest group of health care technicians and practitioners, provide and coordinate patient care. The number of registered nurses in the U.S. increased from roughly 2.68 million in 2010 to approximately 3.41 million in 2021. Interestingly, the percentage of immigrant registered nurses only slightly increased from 2007 to 2021, from 14.88% to 15.97%.
Figure 6a — Total Registered Nurses in the U.S., 2010-2021
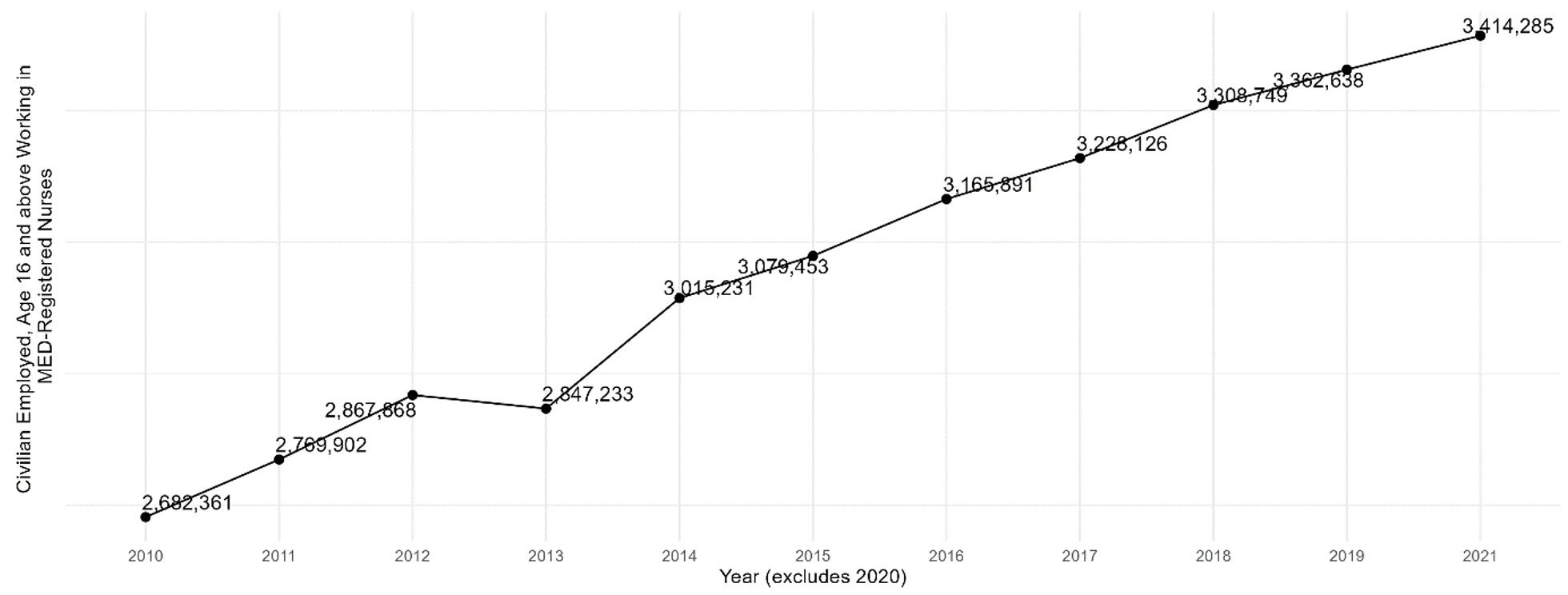
Note Includes workers aged 16 and over. ACS occupational data for nurses was not available for 2007-2009.
Figure 6b — Immigrant Share of Registered Nurses in the U.S., 2010-2021
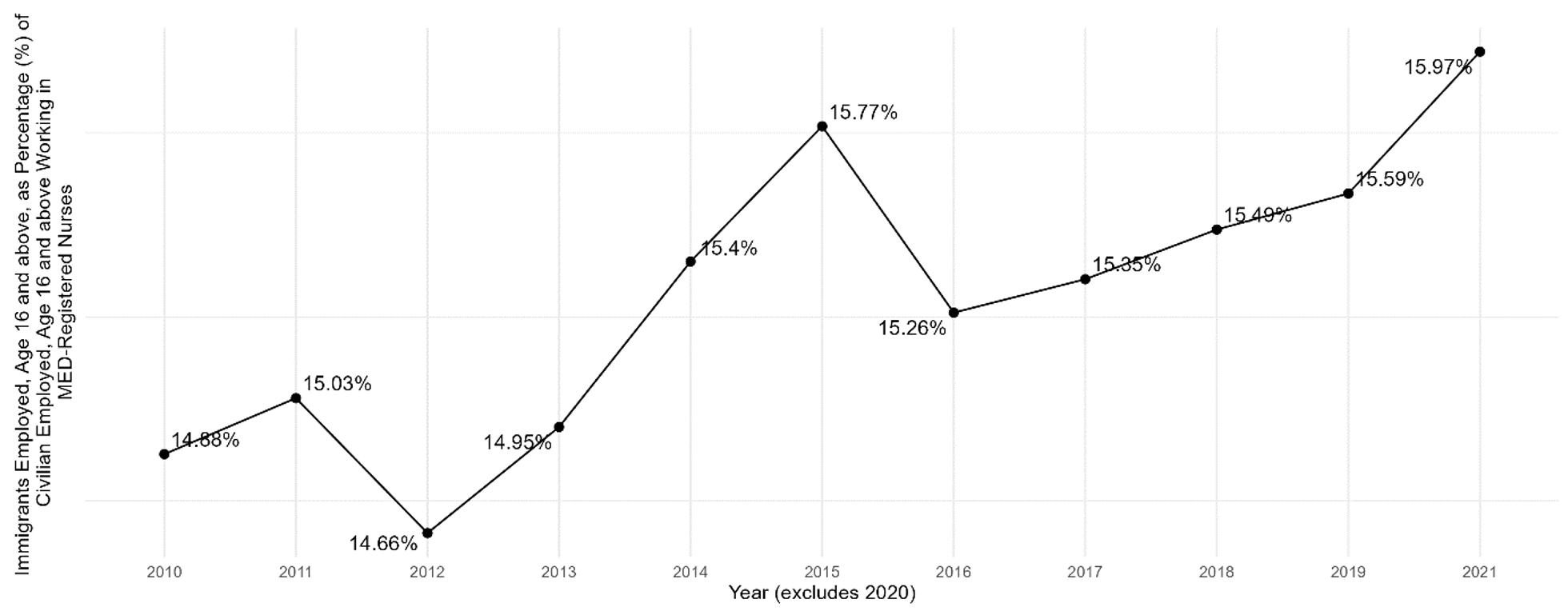
Note Includes workers aged 16 and over. ACS occupational data for nurses was not available for 2007-2009.
Despite the growing number of physicians and surgeons, illustrated in Figure 7a, a study by Markit (2021) estimates that the United States may face a shortage of 37,800 to 124,000 physicians by 2034, with deficits in both primary and specialty care. Meanwhile, the percentage of immigrant physicians consistently ranged from 26% to 28% between 2007 and 2019; in 2021, it reached a low of 26.47%.[3]
Figure 7a — Total Physicians and Surgeons in the U.S., 2007-2021
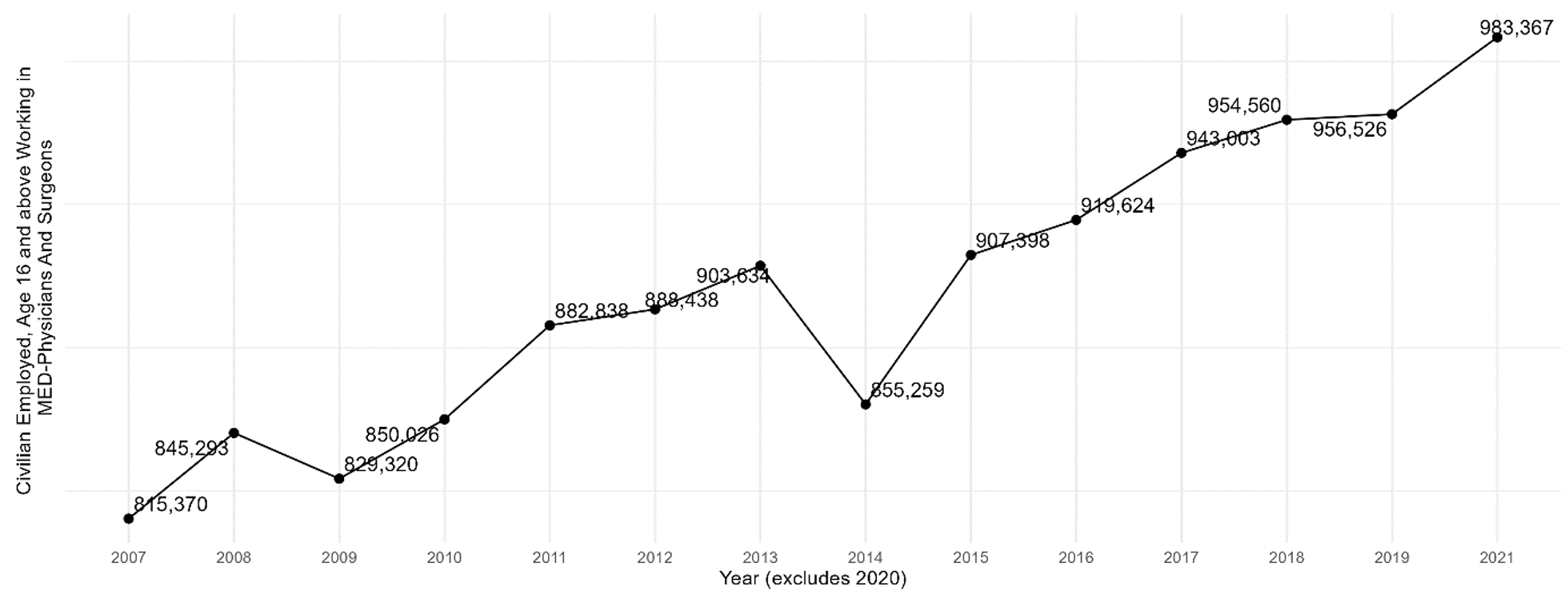
Note Includes workers aged 16 and over.
Figure 7b — Immigrant Share of Physicians and Surgeons in the U.S., 2007-2021
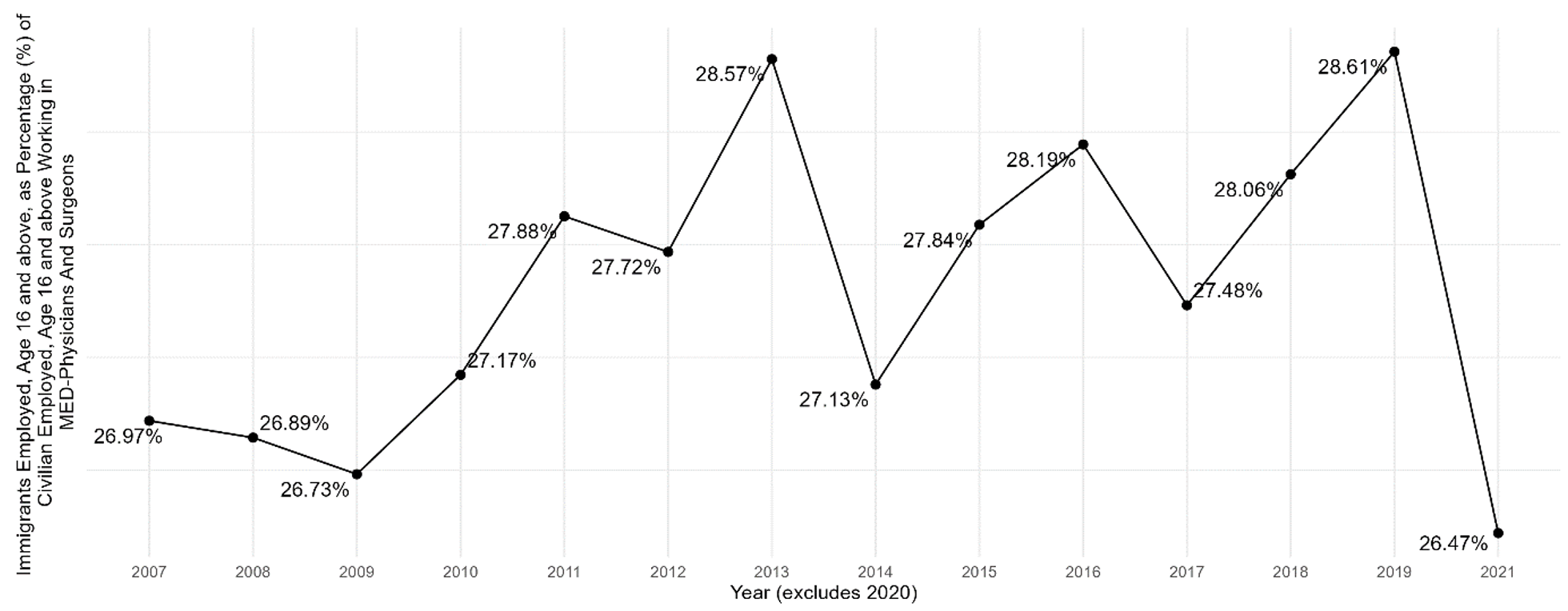
Note Includes workers aged 16 and over.
Figure 8 demonstrates the growth in the number of nursing psychiatric and home health aides, a thriving occupation in the health care support industry. Home health aides are trained health care professionals who assist individuals who have disabilities or chronic illnesses or who need additional support in their homes. It is important to distinguish between home health aides and other home health workers like home health nurses, physical therapists, and occupational therapists, who are required to undergo specialized training and certifications to provide medical and skilled care.
The demand for home health aides has significantly increased due to the aging population of baby boomers, who were born between 1946 and 1964. This demand was further fueled by Medicare’s expansion of coverage for home health services in 2017, which facilitated greater access to the benefits of home health aides.
Figure 8a — Total Number of Nursing, Psychiatric, and Home Health Aides in the U.S., 2007-202
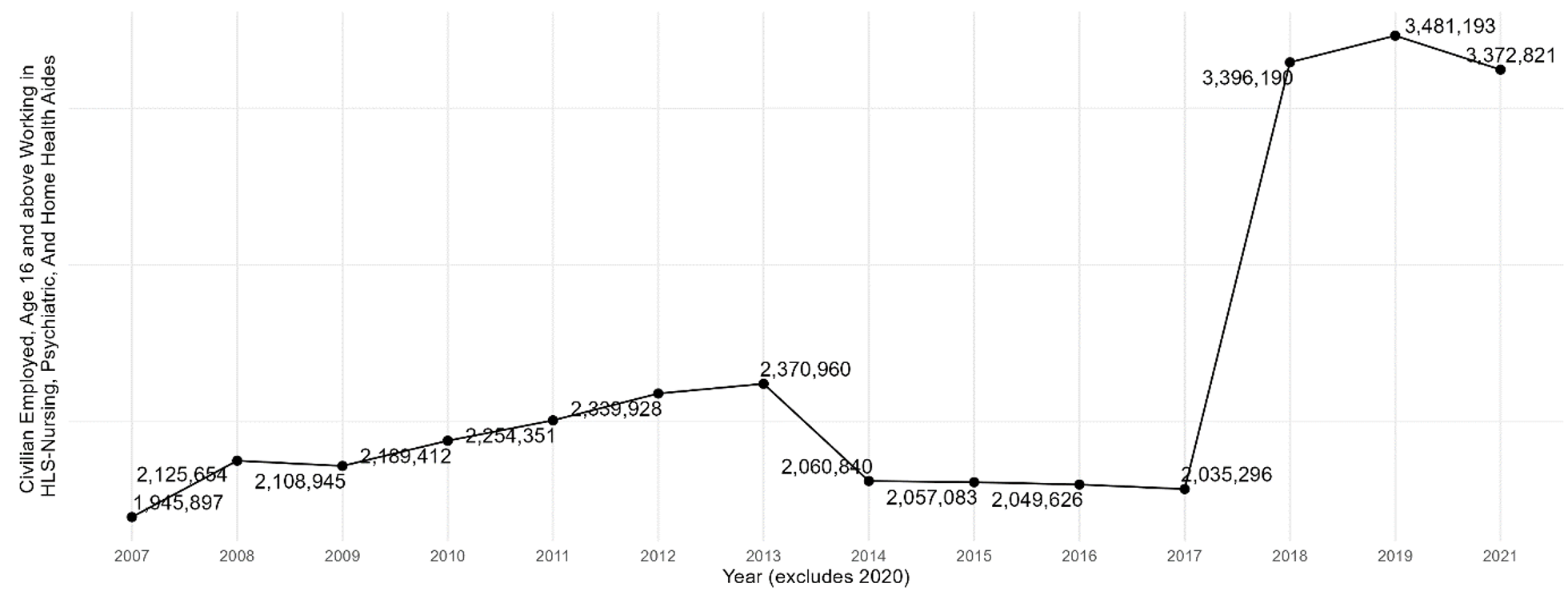
Note Includes workers aged 16 and over.
Figure 8b — Immigrant Share of Nursing, Psychiatric, and Home Health Aides in the U.S., 2007-2021
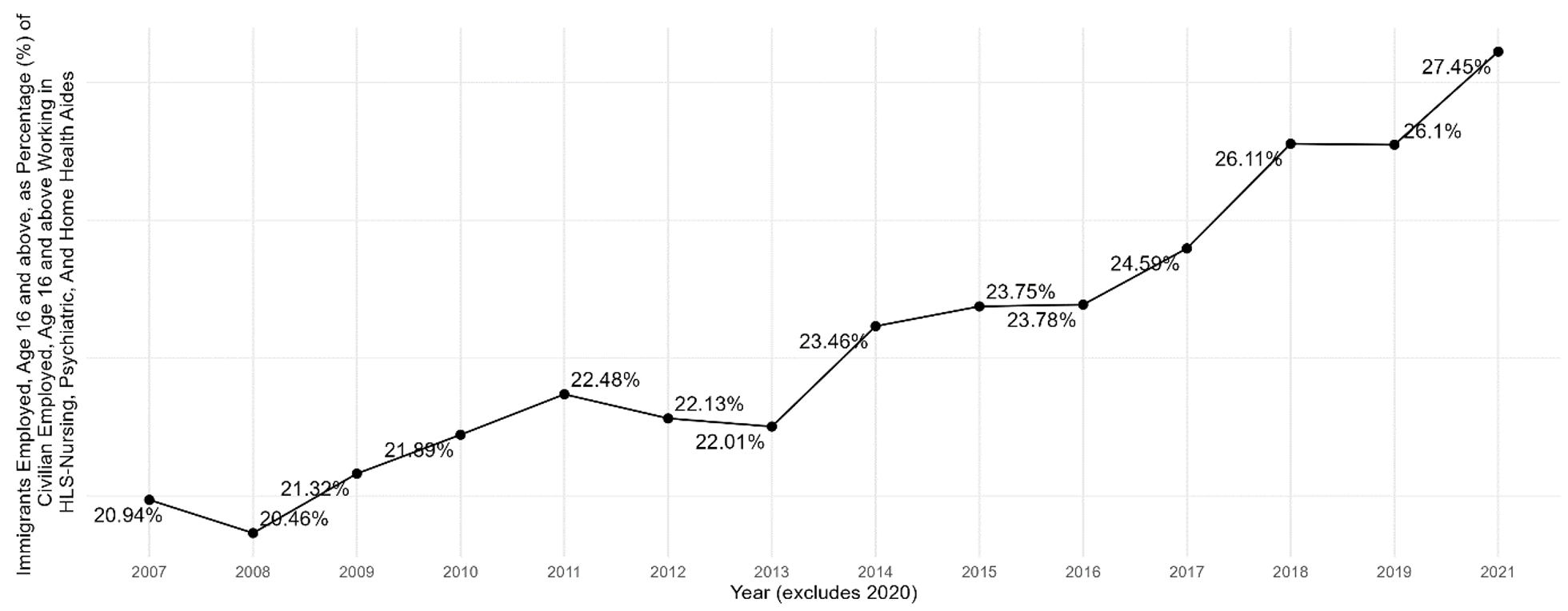
Note Includes workers aged 16 and over.
According to the BLS, the median annual income for home health and personal care aides was $29,430 in 2021. The BLS projects a significant growth of 25.4% for this occupation between 2021 and 2031, positioning it as one of the occupations with the highest job growth. Notably, the percentage of immigrants working in this field increased from 19.2% in 2007 to 26% in 2021.
Discussion
Projection
The BLS has projected that employment will grow from 162.8 million to 168.8 million from 2019-2029, an increase of 6 million jobs (U.S. Bureau of Labor Statistics, “News Release”). This reflects an annual growth rate of 0.4%, slower than the 2009-19 annual growth rate of 1.3%. Five out of the 20 industry groups projected to have the fastest growth from 2019 to 2029 belong to the health care and social assistance sector (U.S. Bureau of Labor Statistics, “5 out of 20”). These industry groups are individual and family services, home health care services, outpatient care services, offices of other health practitioners, and other ambulatory health care services. The significant increase in available positions in the health care and social assistance sector is expected to be driven by various factors, such as the aging baby boomer population, longer life expectancy, continued growth in the number of patients with chronic conditions, increased demand for preventive care, and the adoption of new technologies in health care. Among these industry groups, health care occupations and those associated with health care (including mental health) make up most of the 20 occupations projected to grow the fastest from 2019 to 2029. The occupations with the fastest-projected growth rates include nurse practitioners, occupational therapy assistants, physician assistants, home health aides, and personal care aides.
Health Care Provider Shortages
There is a chronic shortage of health care providers in the United States. This shortage is attributed to several factors, including the aging population, the growing demand for health care services, and the retirement of baby boomers. The shortage has resulted in various adverse consequences, such as longer patient wait times, reduced access to care, and increased costs. Rural areas and hospitals that cater to low-income patients are particularly affected by this shortage.
To address the health care worker shortage, the American Hospital Association (AHA 2021) suggests implementing strategies such as increasing pay and benefits for health care workers, expanding training programs, and recruiting foreign workers.
Immigrant Health Care Providers
Immigrants help alleviate the current shortage of health care professionals through multiple avenues, as highlighted in a report by the AHA (2021). First, immigrants are more likely than native-born Americans to work in health care. According to the report, immigrants accounted for 18.2% of all health care workers in the United States in 2017, compared to 13.7% in the general workforce. Second, immigrants appear more inclined to pursue high-demand health care occupations like nursing and home health care. In 2017, for example, immigrants comprised 27.5% of all registered nurses in the United States, while representing only 16.4% of the general workforce. Third, immigrants are more likely to work in rural areas, where health care worker shortages are prevalent. In 2017, immigrants represented 22.4% of all health care workers in rural areas, compared to 18.2% in urban areas (AHA 2021).
In 2016, out of the 974,449 doctors practicing in the United States, around 25% (approximately 247,449) were foreign-trained. Among these foreign-trained doctors, 59% specialized in primary care fields, and 30% practiced in medically underserved areas. By comparison, U.S.-trained doctors accounted for 45% and 21%, respectively, in those categories (American Immigration Council 2018). This evidence suggests that roughly one-quarter of all practicing physicians opt to work in primary care fields, particularly in underserved communities, and that immigrant doctors are more likely to do so.
U.S. immigration policies impose significant limitations on the ability of foreign-trained health care professionals to immigrate to and practice in the United States. For example, the H-1B visa, a nonimmigrant visa that temporarily enables U.S. employers to employ foreign workers in specialty occupations and the most common visa for foreign-trained doctors, has an annual cap of 65,000. Since 2008, this cap has been reached yearly, preventing many qualified foreign-trained doctors from obtaining visas to the United States.
The United States has implemented other various programs to recruit foreign workers and address health care provider shortages, including the J-1 Visa Exchange Visitor Program, the Conrad 30 Waiver Program, the H-2B Temporary Non-Agricultural Worker Program, nurse immigration programs, state-based initiatives, and visa recapture proposals. These are discussed in further detail below.
Foreign medical doctors can apply for U.S. medical residency programs through the Electronic Residency Application Service (ERAS), which can provide applicants with a J-1 visa for residency training in the U.S., and through the National Resident Matching Program (NRMP). After completing their residency, these doctors may apply for a work visa or pursue a further specialization. Currently, however, the number of medical school graduates within the U.S. exceeds the number of residency positions available (Boyle 2023), limiting foreign doctors’ ability to take advantage of these programs.
The Exchange Visitor Program (EVP), also known as the J-1 visa, presents an alternative path for international candidates to travel to and gain experience in the United States through participation in work- and study-based programs. The purpose of the J-1 Exchange Visitor Program is to “increase mutual understanding between the people of the United States and the people of other countries by means of educational and cultural exchanges” (Citizenship and Services 2023). Upon completing the program, J-1 visa-holding foreign nationals must in most cases return home for two years before returning to the U.S. on either a nonimmigrant visa or as a lawful permanent resident. This requirement — or 212(e), as it is referenced in the immigration regulations — stipulates that those who come to the U.S. with J-1 status cannot become lawful permanent residents in the U.S., change status in the U.S., or get work or family-based U.S. visa statuses such as H, L, or K until they return to their country of last permanent residence for at least two years cumulatively (The Office of International Affairs 2023).
J-1 visa waiver programs allow foreign nationals to waive the requirement to return home for two years before returning to the U.S. The Conrad 30 Waiver Program, for example, enables J-1 visa-holding foreign medical graduates (FMGs) to waive the requirement as part of an effort to improve access to qualified medical doctors in federally designated health professional shortage areas (HPSAs). U.S. Citizenship and Immigration Services (2020) details the waiver’s eligibility criteria for J-1 visa-holding foreign medical graduates, including the stipulation that applicants secure full-time medical employment for at least three years in an HPSA, medically underserved area (MUA), or community with a medically underserved population (MUP). Applicants also must submit a written “no objection” statement if required to return to their home country and must start their employment within 90 days of receiving the waiver, not upon the J-1 visa’s expiration. In addition to these eligibility criteria, each state has developed its own waiver application rules and guidelines.
If foreign medical doctors actively practicing in their home country want to serve patients in the U.S., they generally must repeat their residency training in an accredited residency program in the U.S. and pass the standardized U.S. medical licensing exam. These requirements deprive many residents of competent care from experienced physicians (Singer 2023). To address his state’s growing physician shortage, in May 2023 Tennessee Gov. Bill Lee signed H.B. 1312 into law to remove redundant medical residency requirements for foreign-trained doctors in good standing. [4] These doctors must show equivalent training, pass identical exams, be fully licensed in good standing in another country, and have practiced medicine abroad without incident. Additionally, they must be sponsored and employed by a residency-training health care provider, and after two years of successful and safe practice, automatically receive a full Tennessee medical license (Wolfson 2023).
According to Martin et al. (2023), nearly 800,000 nurses are projected to exit the workforce by 2027 due to stress, burnout, and retirement. This forecast follows the resignation of approximately 100,000 registered nurses during the COVID-19 pandemic. The National Council of State Boards of Nursing (NCSBN), a nonprofit organization focused on nursing regulations, found in its 2022 National Nursing Workforce Survey that registered nurses with less than 10 years of experience accounted for approximately 41% of registered nurses who left the profession during the pandemic.
Some health systems have bolstered their international recruitment efforts or partnered with nursing schools to improve the workforce pipeline and combat the ongoing nursing shortage. For example, Henry Ford Health has planned to bring in 500 nurses from the Philippines, similar to what the institution did in the 1990s and 2000s. AdventHealth, a Florida-based health system, expects to hire over 400 foreign-born nurses in 2023, up from 280 in 2022 (Young and White 2023).
Conclusion
The percentage of foreign-born individuals in the United States is increasing, and as a result, immigrants hold a significant proportion of jobs in the civilian workforce, especially in health care and social assistance. Some health care and social assistance subsectors, such as nursing and residential care facilities, and industry groups, such as child day care services and vocational rehabilitation services, are experiencing a decline. However, the overall number of immigrants employed in the health care and social assistance sector continues to increase, highlighting the critical role immigrants play in the United States workforce and particularly in health care.
Programs like the Conrad 30 Waiver Program, legislation like Tennessee H.B. 1312, and the international recruitment of nurses are notable efforts to capitalize on the capacity of immigrants to reduce worker shortages and improve access to care for rural and medically underserved areas. However, visa processes are too slow and costly to fully match the demand for foreign health care providers in the United States. Addressing these barriers and embracing and integrating immigrant health care workers should be part of a strategic response to the critical challenges facing the U.S. health care sector.
Appendix A: Health Care
Figure A1.1 — Total Number of Workers in U.S. Physician Offices, 2007-2021
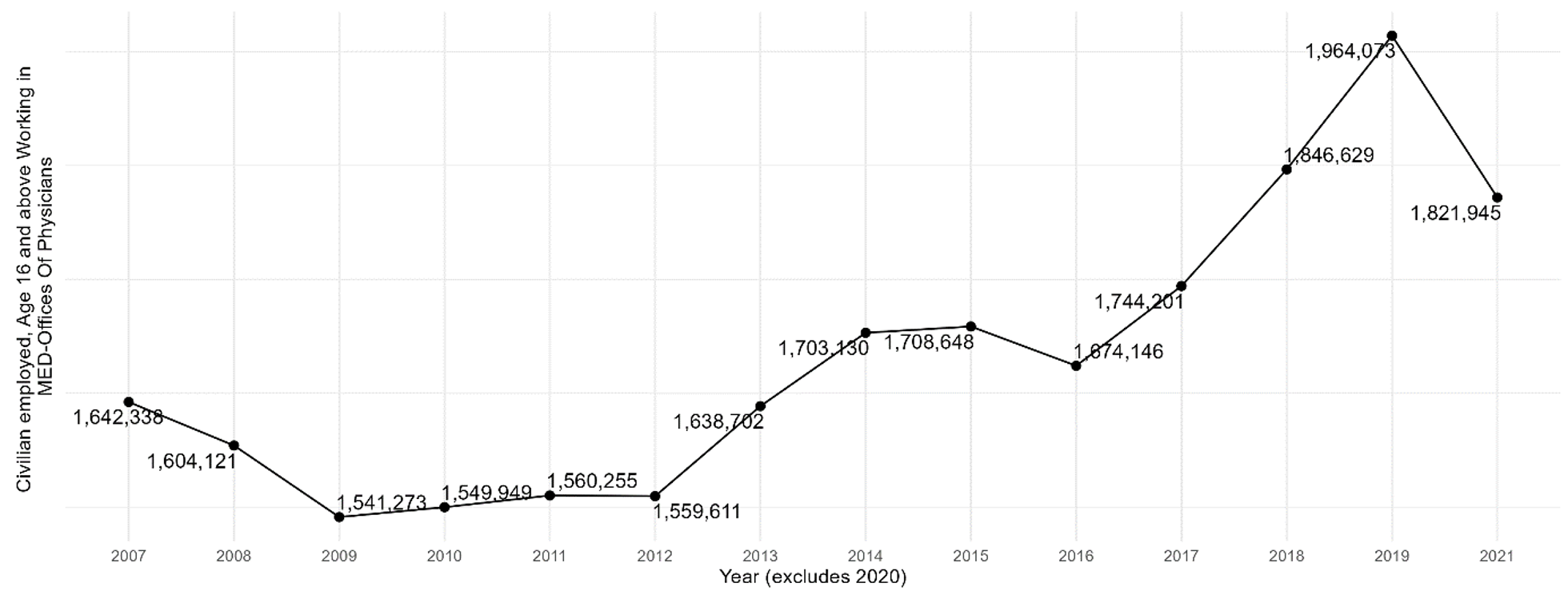
Note Includes workers aged 16 and over.
Figure A1.2 — Immigrant Share of Workers in U.S. Physician Offices, 2007-2021
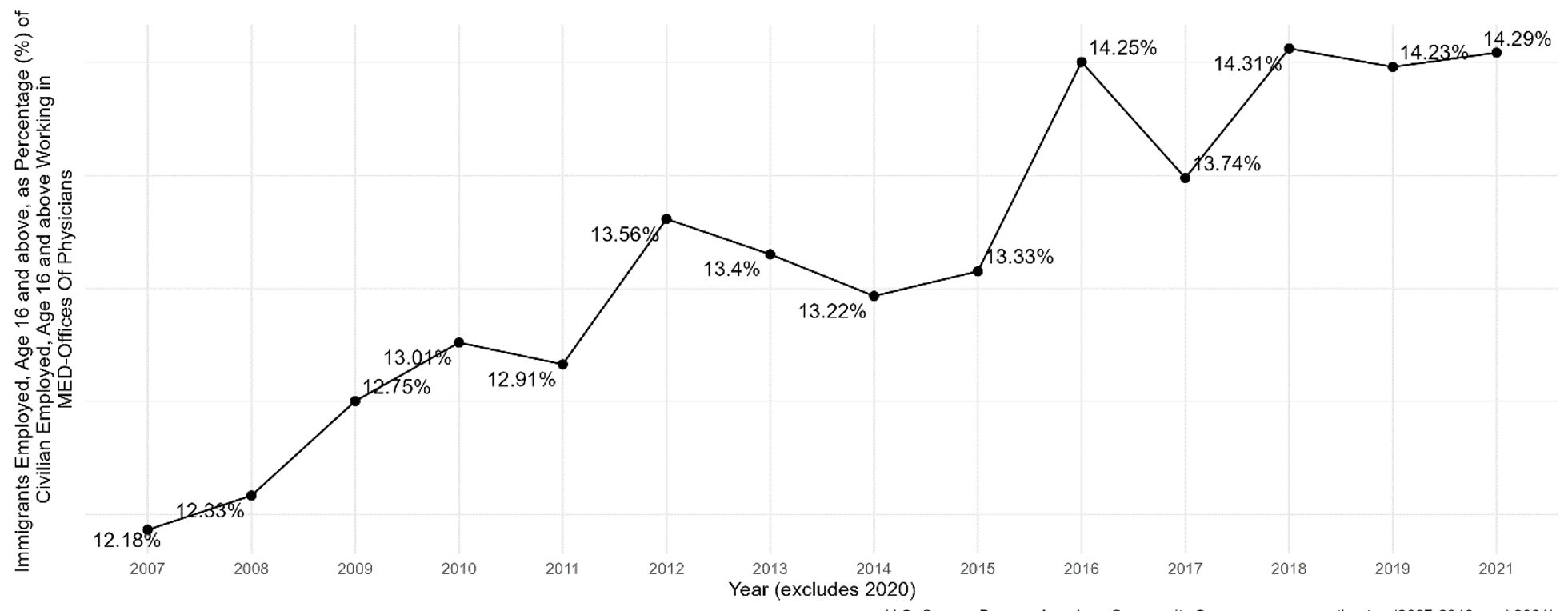
Note Includes workers aged 16 and over.
Figure A2.1 — Total Number of Workers in U.S. Hospitals, 2007-2021
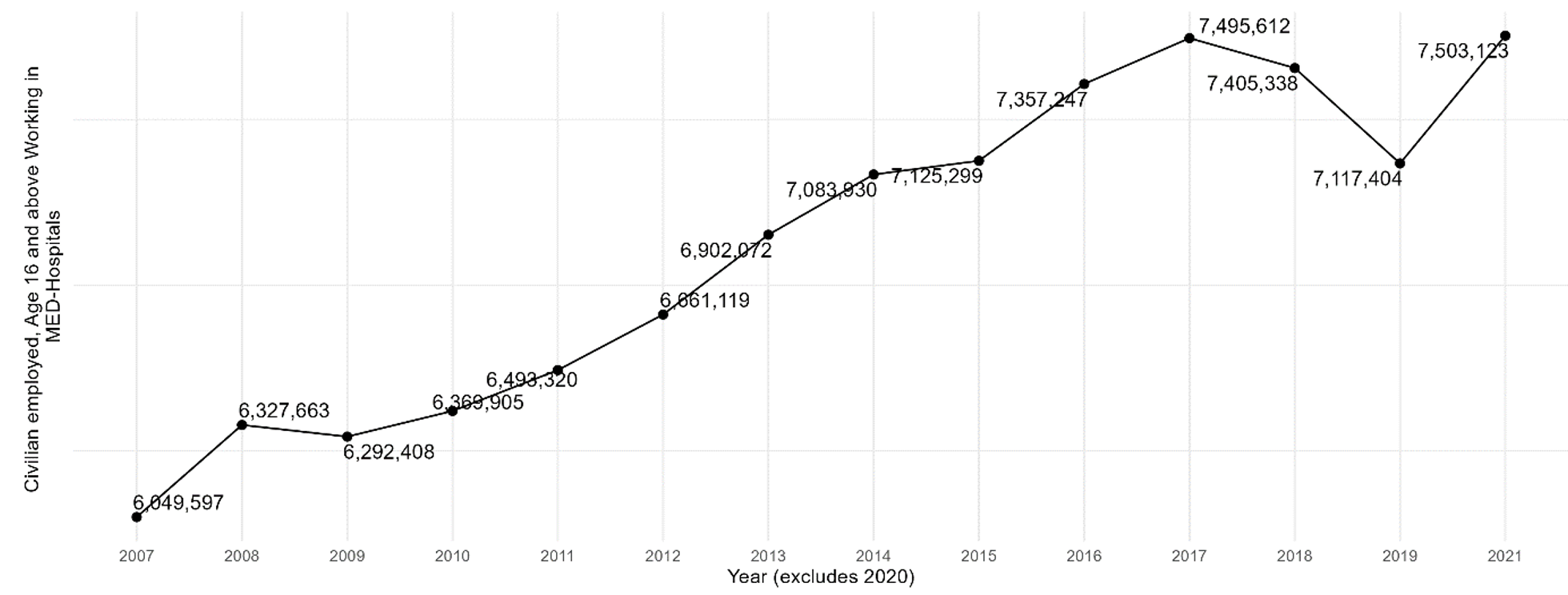
Note Includes workers aged 16 and over.
Figure A2.2 — Immigrant Share of Workers in U.S. Hospitals, 2007-2021
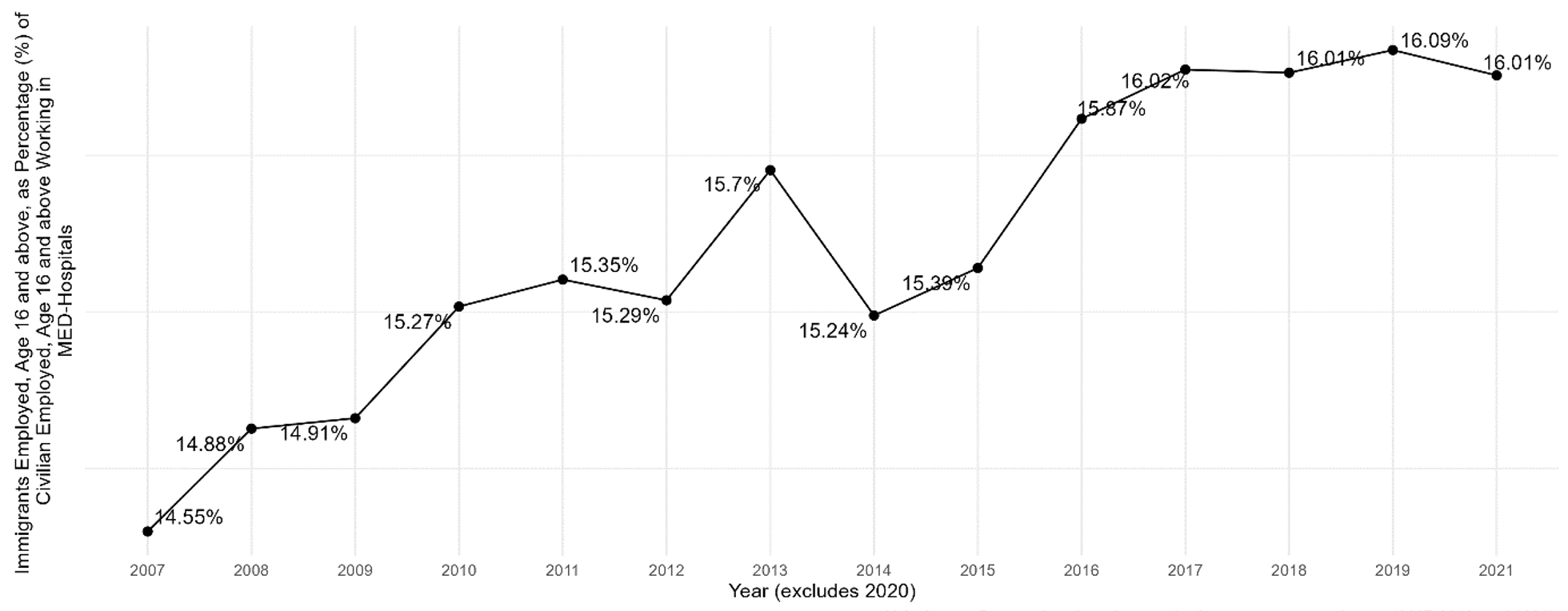
Notes Includes workers aged 16 and over. Hospitals comprise general medical, surgical, and specialty (including psychiatric and substance abuse) hospitals.
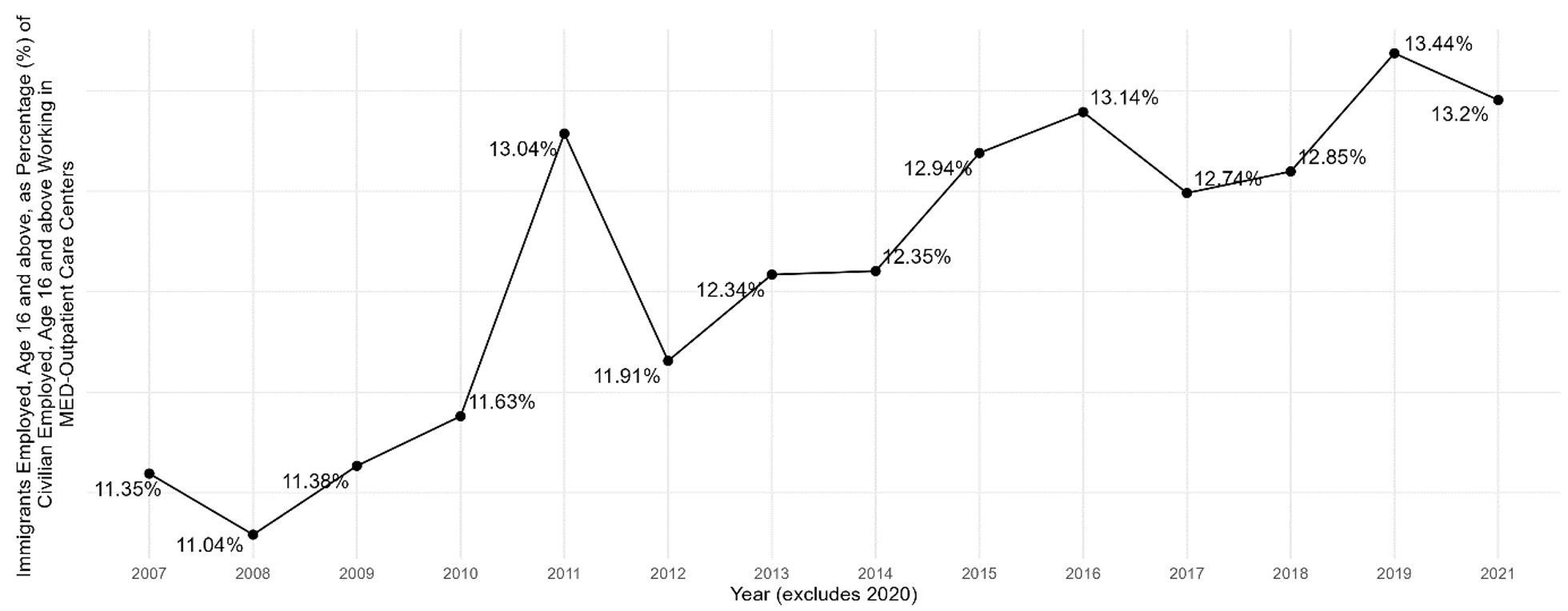
Figure A3.1 — Total Number of Workers in U.S. Outpatient Care Centers, 2007-2021
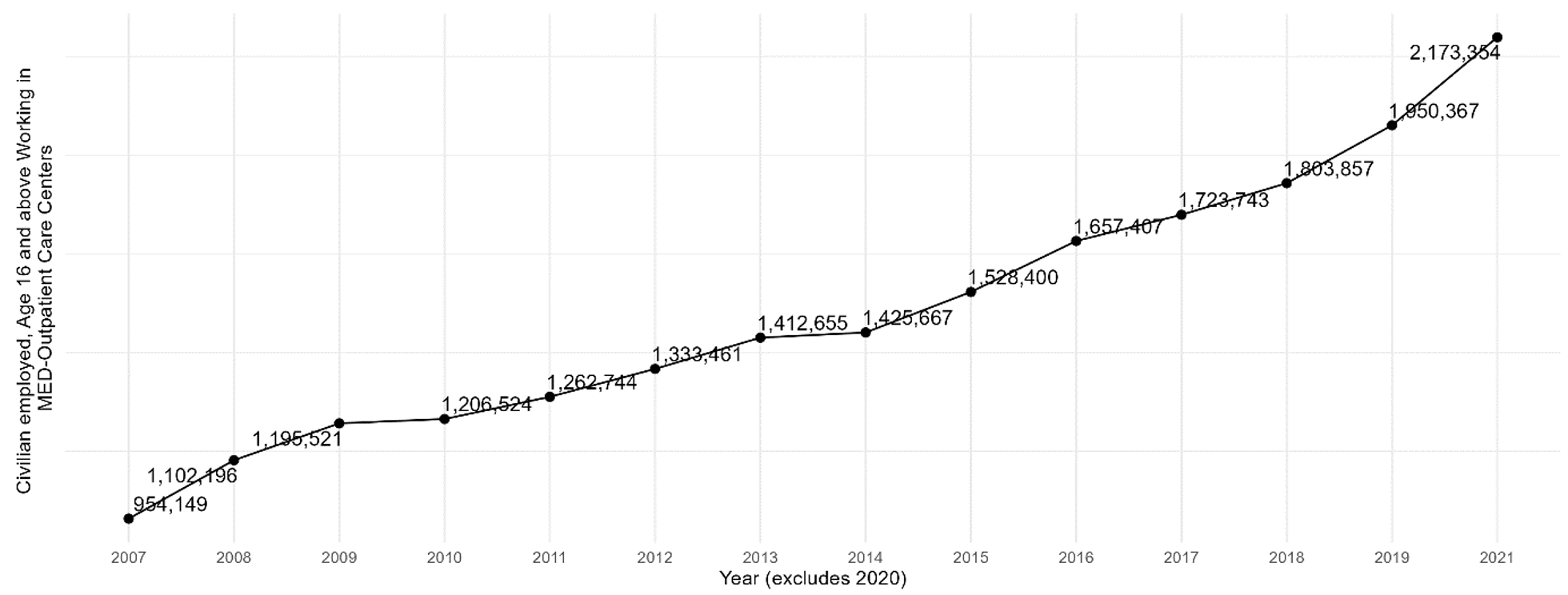
Note Includes workers aged 16 and over.
Figure A3.2 — Immigrant Share of Workers in U.S. Outpatient Care Centers, 2007-2021
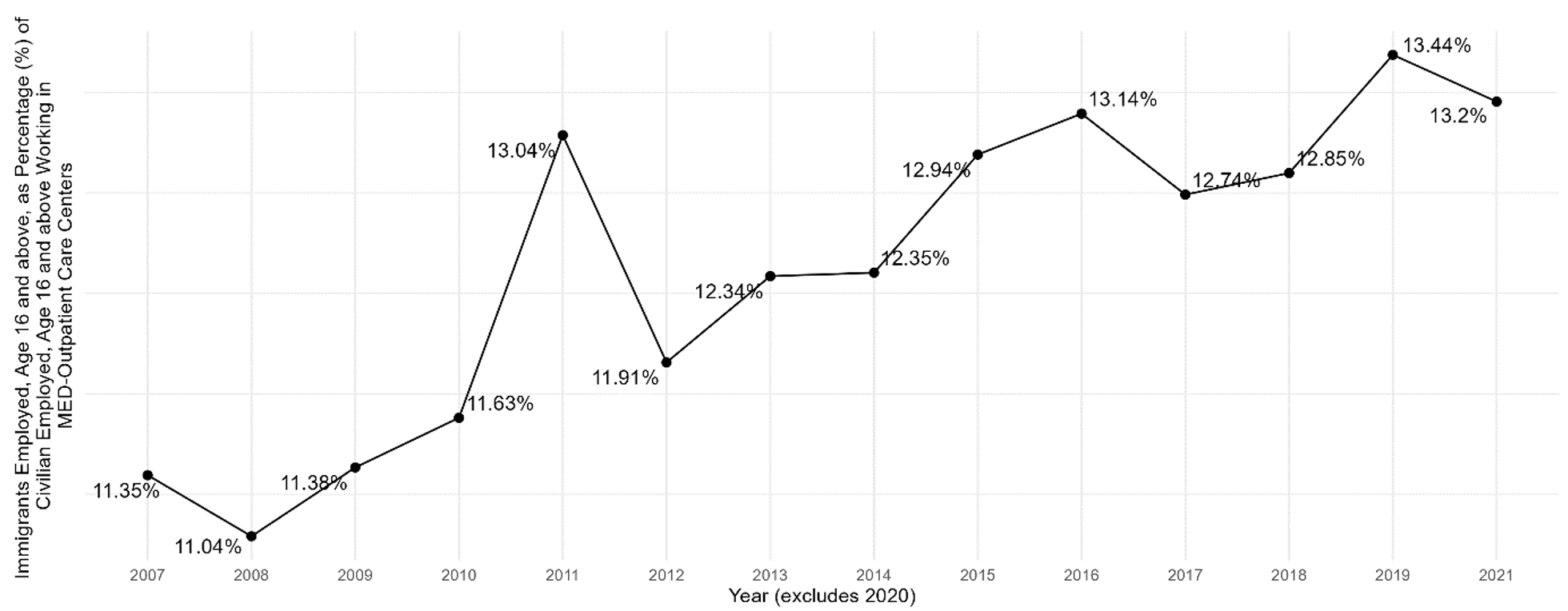
Note Includes workers aged 16 and over.
Figure A4.1 — Total Number of Workers in U.S. Nursing Care Facilities, 2007-2021
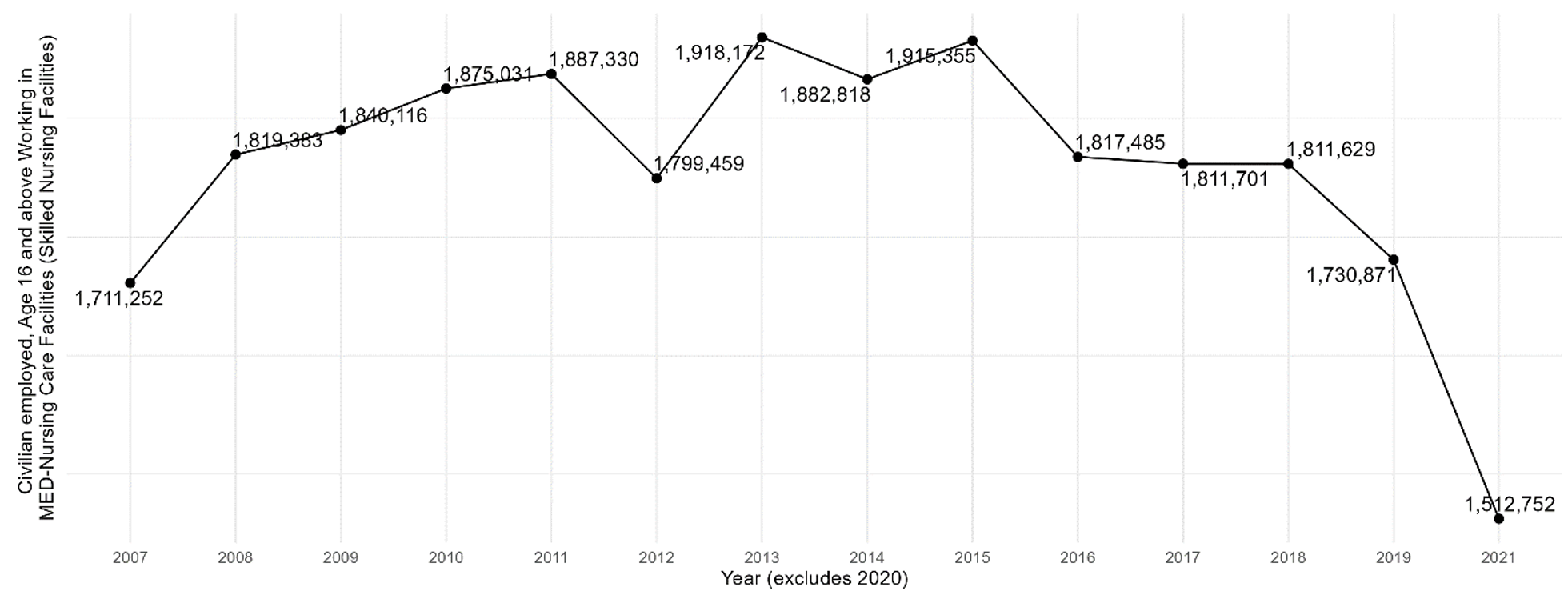
Note Includes workers aged 16 and over; excludes residential care facilities.
Figure A4.2 — Immigrant Share of Workers in U.S. Nursing Care Facilities, 2007-2021

Note Includes workers aged 16 and over; excludes residential care facilities.
Figure A5.1 — Total Number of Workers in U.S. Home Health Care Services, 2007-2021
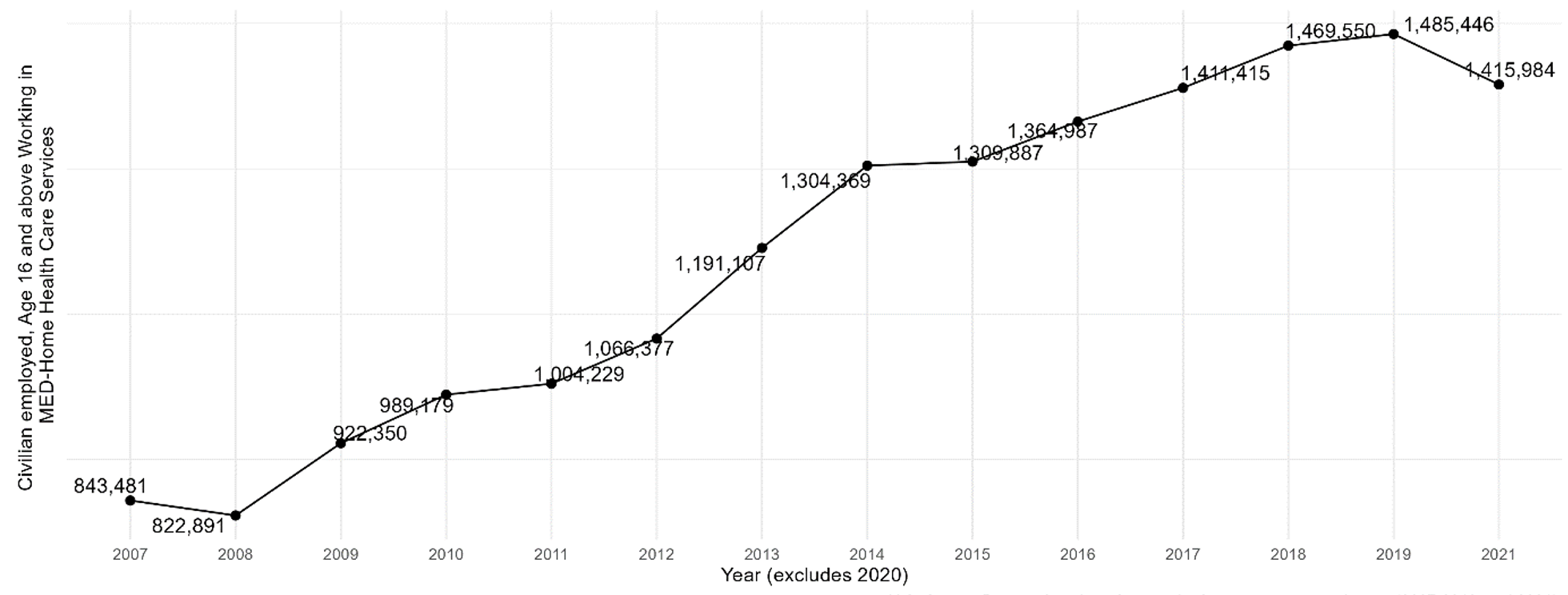
Note Includes workers aged 16 and over.
Figure A5.2 — Immigrant Share of Workers in U.S. Home Health Care Services, 2007-2021
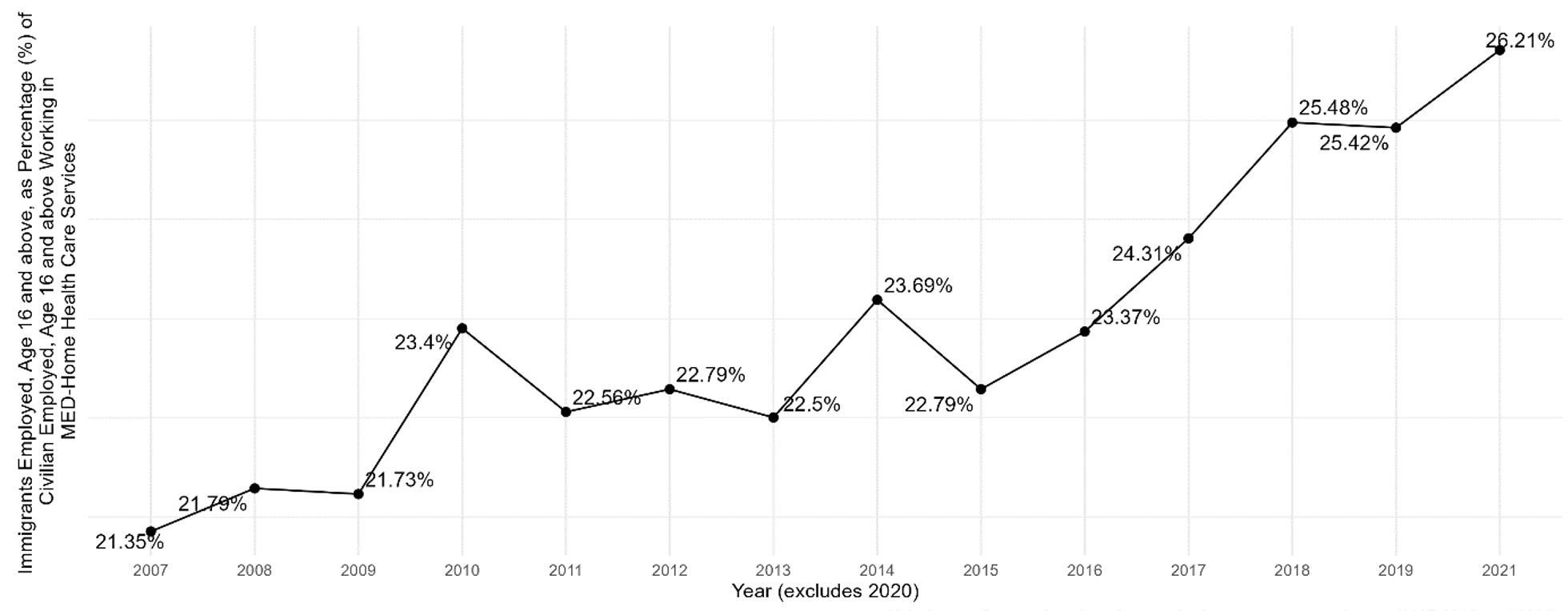
Note Includes workers aged 16 and over.
Figure A6.1 — Total Number of Workers in Other U.S. Health Care Services, 2007-2021
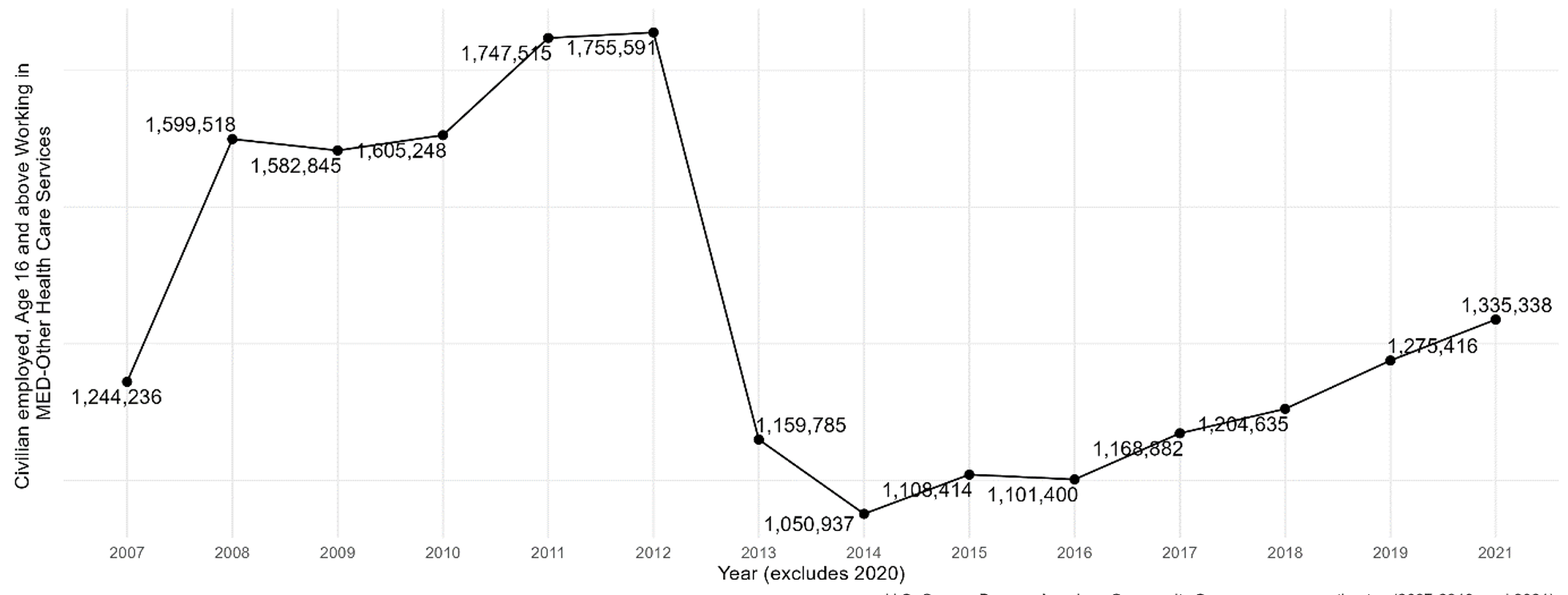
Note Includes workers aged 16 and over.
Figure A6.2 — Immigrant Share of Workers in Other U.S. Health Care Services, 2007-2021
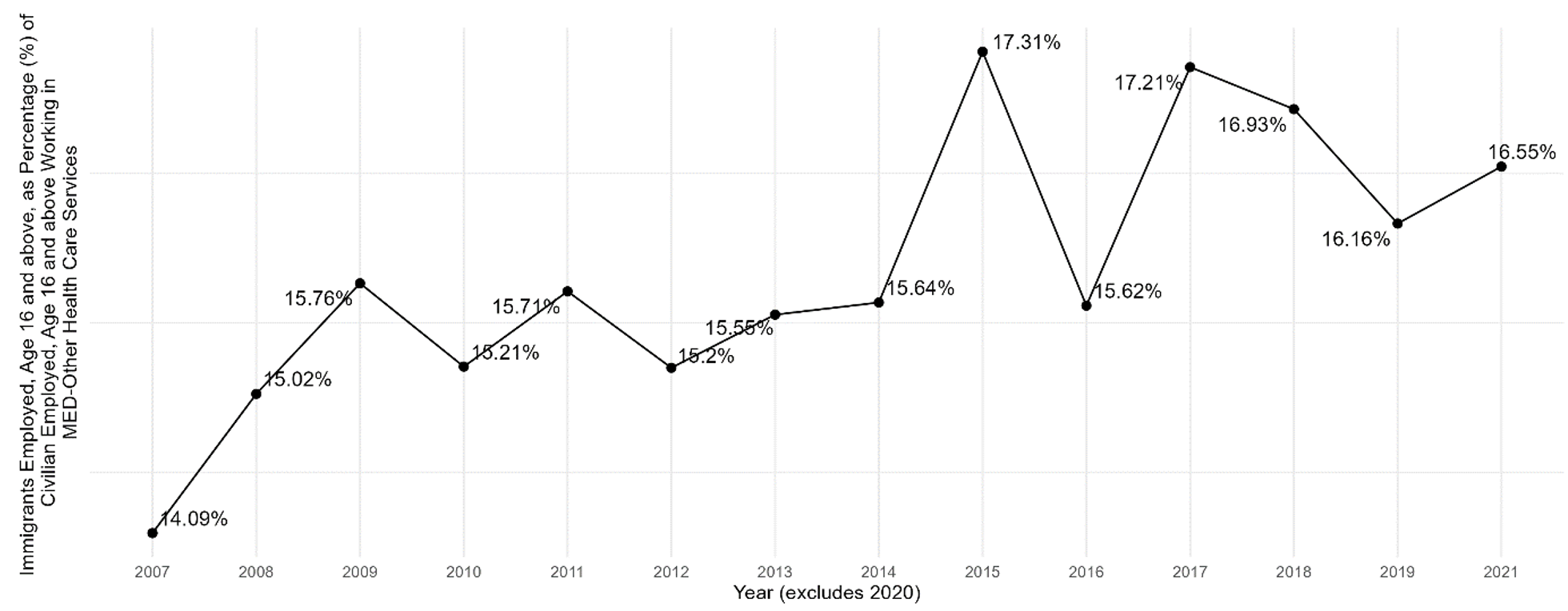
Note Includes workers aged 16 and over.
Figure A7.1 — Total Number of Workers in U.S. Residential Care Facilities, 2007-2021
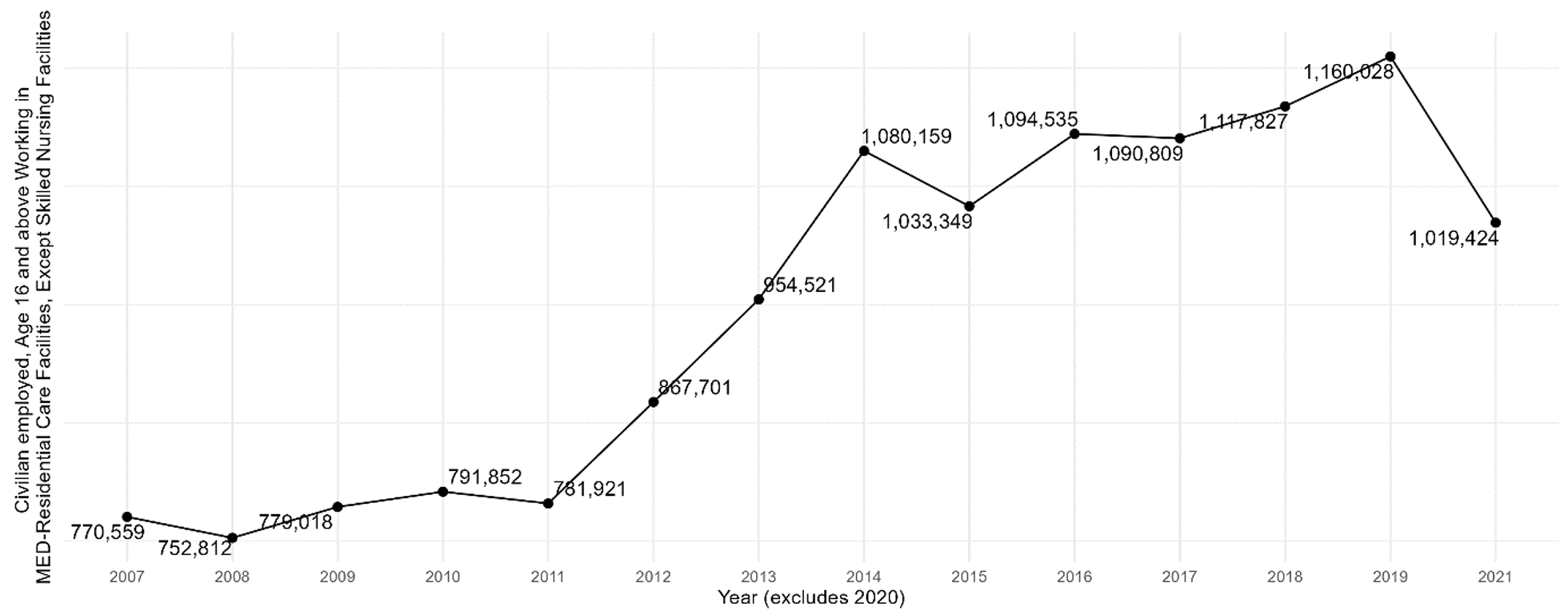
Note Includes workers aged 16 and over; excludes skilled nursing facilities.
Figure A7.2 — Immigrant Share of Workers in U.S. Residential Care Facilities, 2007-2021
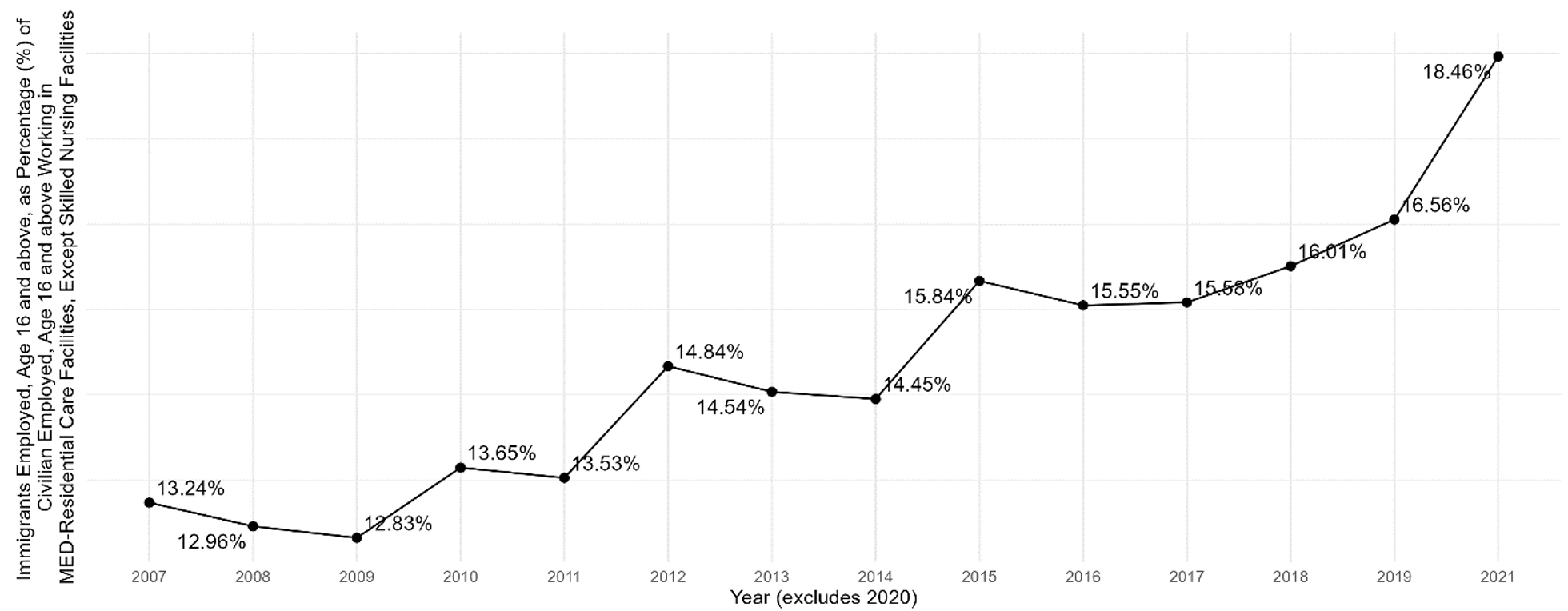
Note Includes workers aged 16 and over; excludes skilled nursing facilities.
Figure A8.1 — Total Number of Workers in U.S. Dentist Offices, 2007-2021
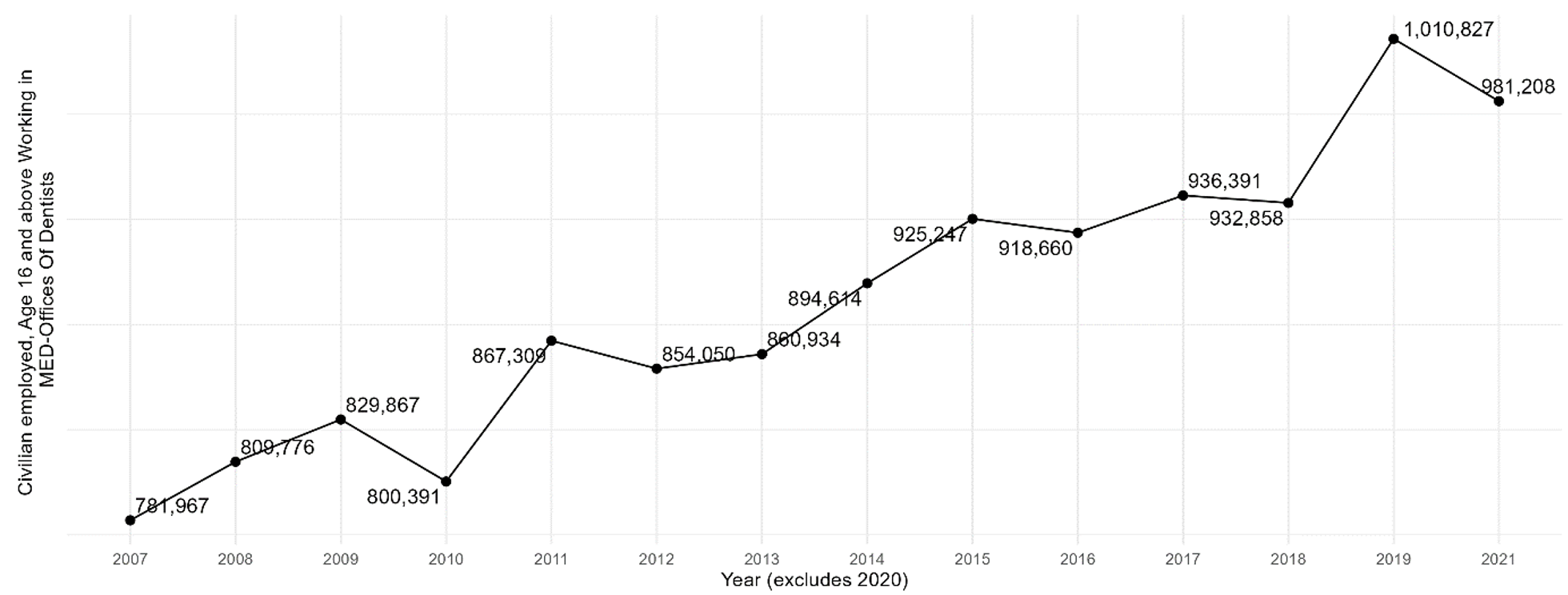
Note Includes workers aged 16 and over.
Figure A8.2 — Immigrant Share of Workers in U.S. Dentist Offices, 2007-2021
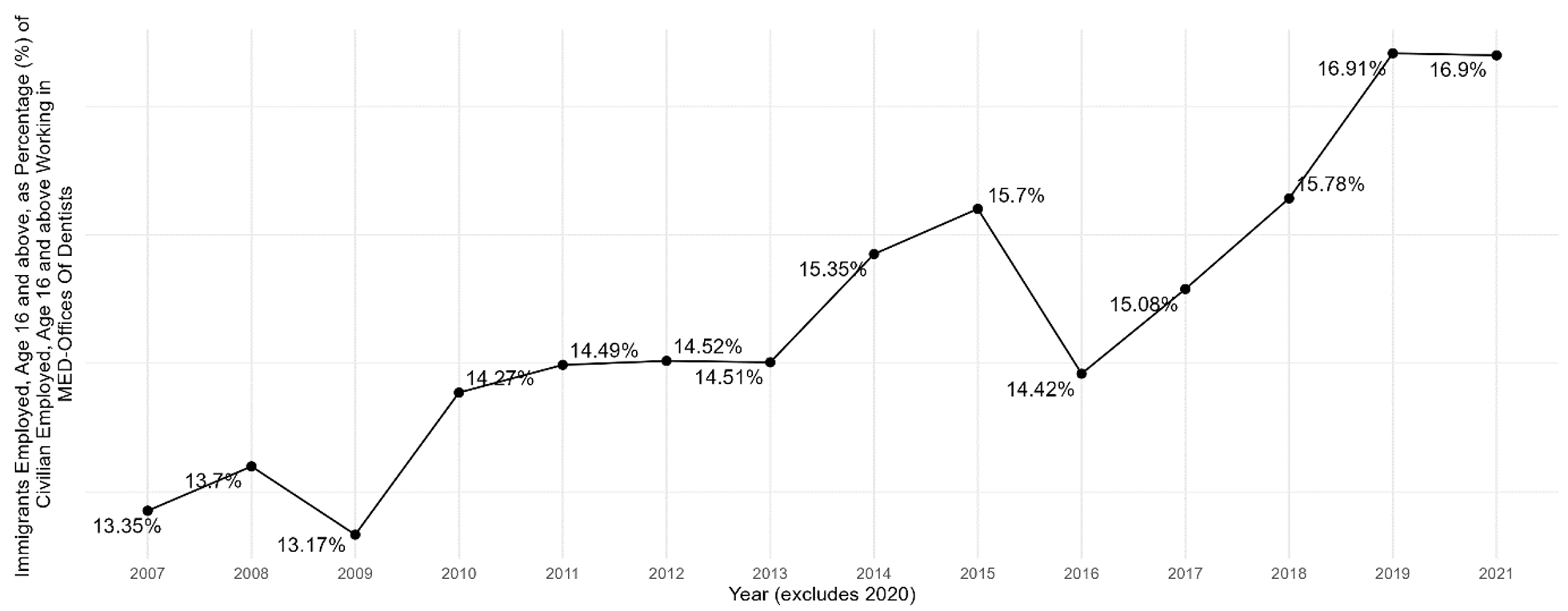
Note Includes workers aged 16 and over.
Figure A9.1 — Total Number of Workers in Other U.S. Health Practitioner Offices, 2007-2021
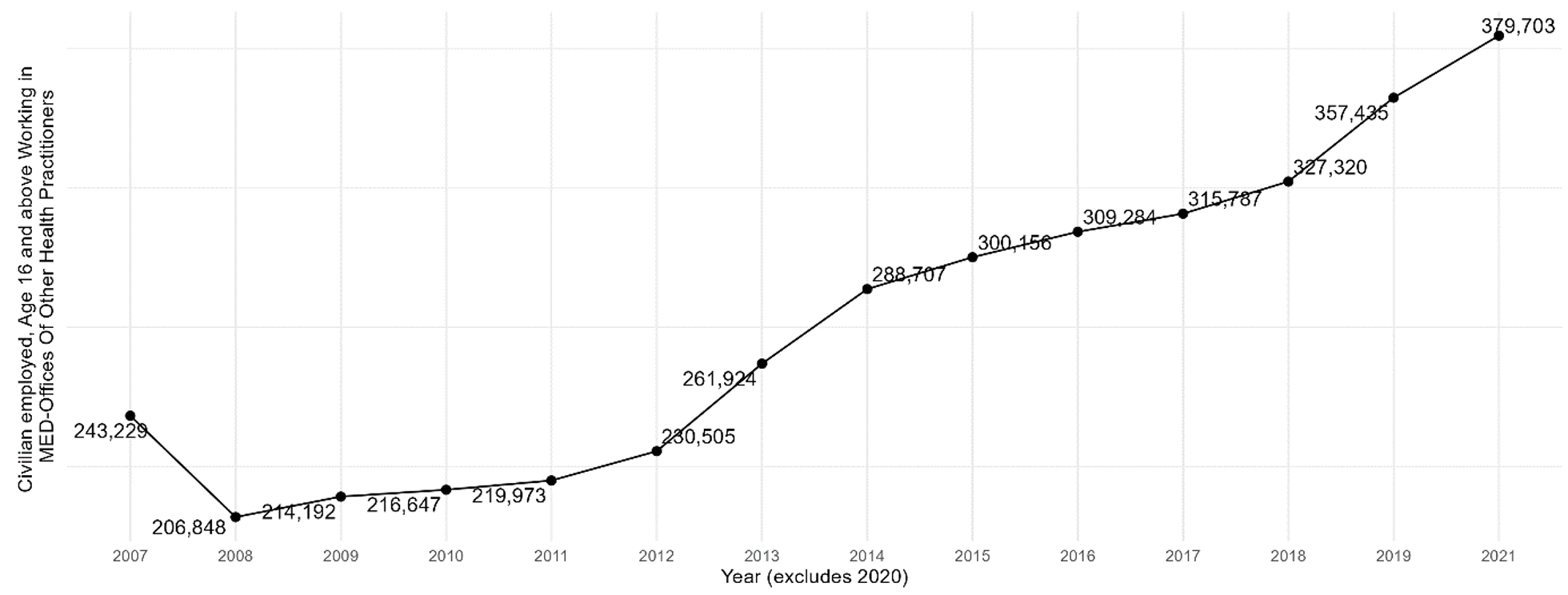
Note Includes workers aged 16 and over.
Figure A9.2 — Immigrant Share of Workers in Other U.S. Health Practitioner Offices, 2007-2021
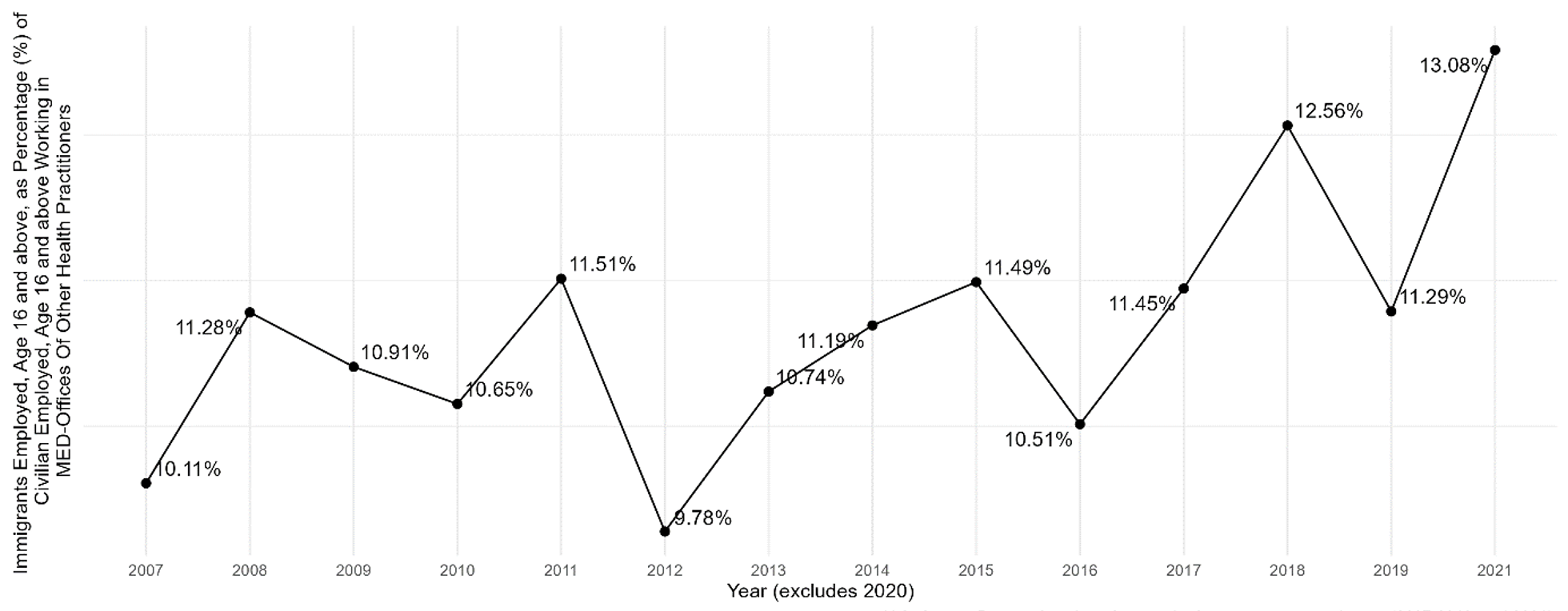
Note Includes workers aged 16 and over.
Figure A10.1 — Total Number of Workers in U.S. Optometrist Offices, 2007-2021

Note Includes workers aged 16 and over.
Figure A10.2 — Immigrant Share of Workers in U.S. Optometrist Offices, 2007-2021
Note Includes workers aged 16 and over.
Appendix B: Social Assistance
Figure B1.1 — Total Number of Workers in U.S. Individual and Family Services, 2007-2021
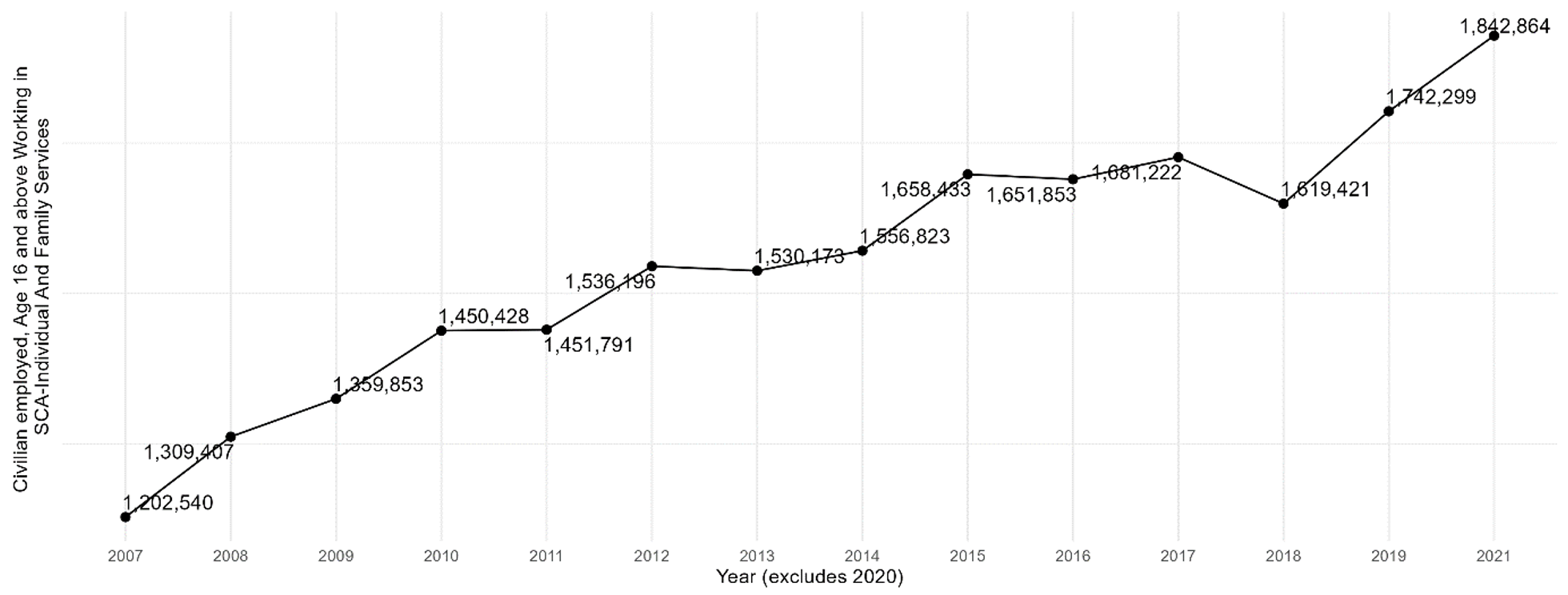
Note Includes workers aged 16 and over.
Figure B1.2 — Immigrant Share of Workers in U.S. Individual and Family Services, 2007-2021
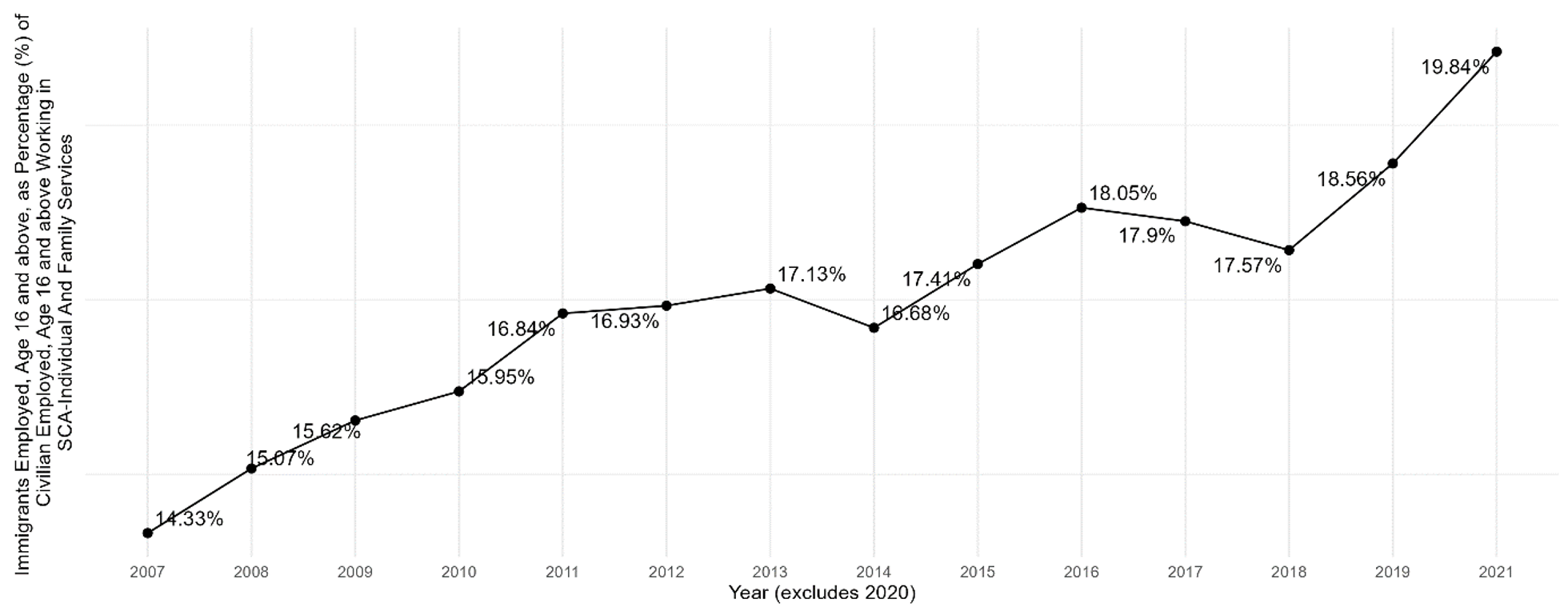
Note Includes workers aged 16 and over.
Figure B2.1 — Total Number of Workers in U.S. Child Day Care Services, 2007-2021
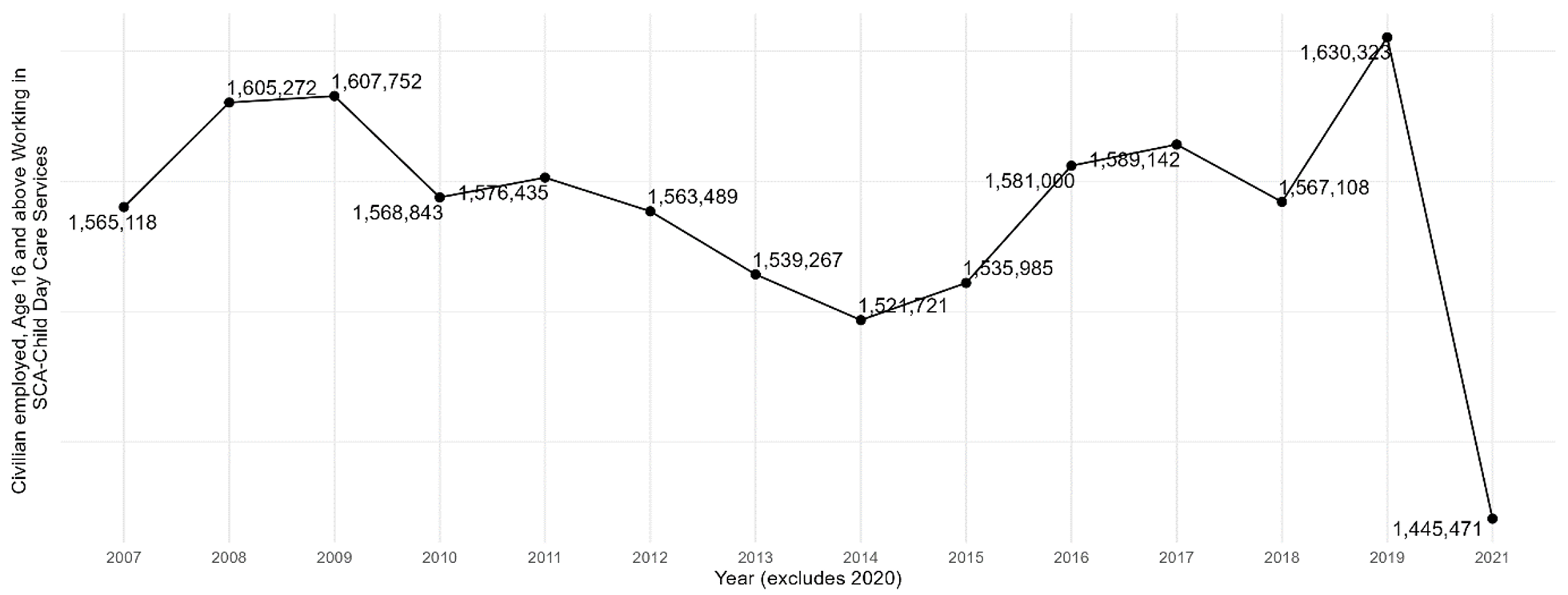
Note Includes workers aged 16 and over.
Figure B2.2 — Immigrant Share of Workers in U.S. Child Day Care Services, 2007-2021
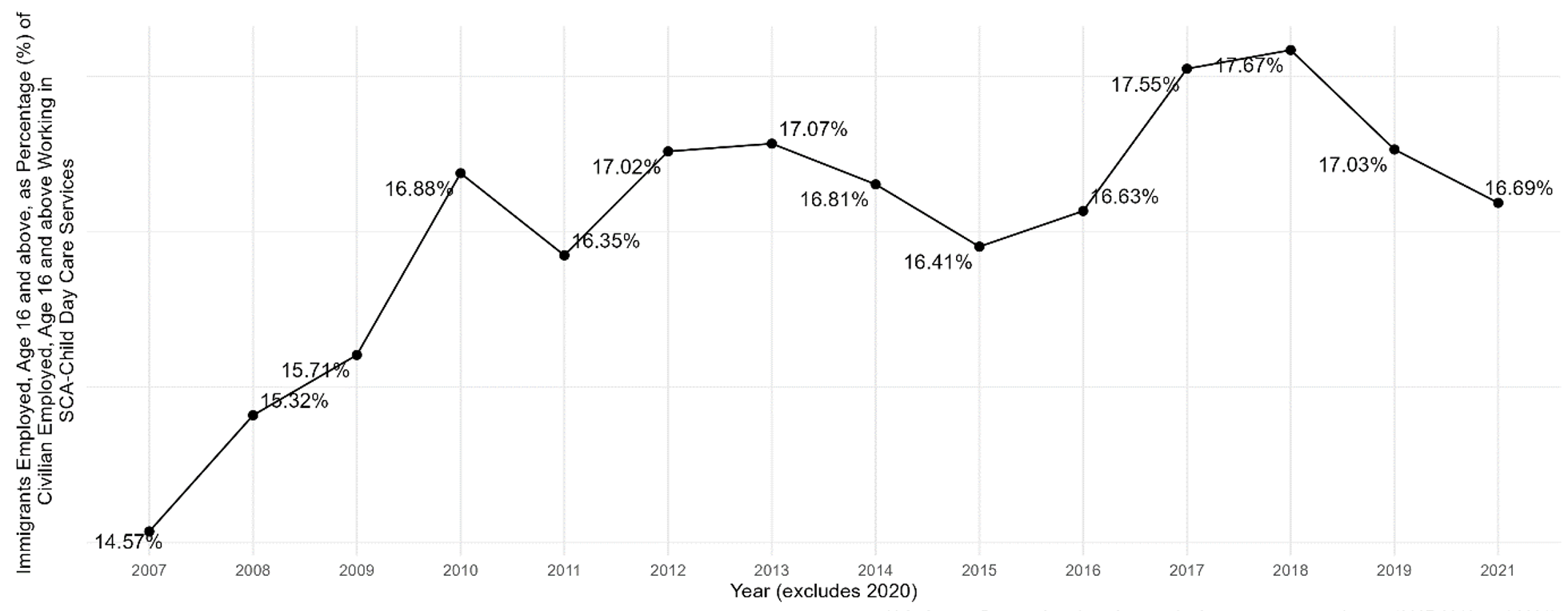
Note Includes workers aged 16 and over.
Figure B3.1 — Total Number of Workers in U.S. Community Food and Housing and Emergency Services, 2007-2021
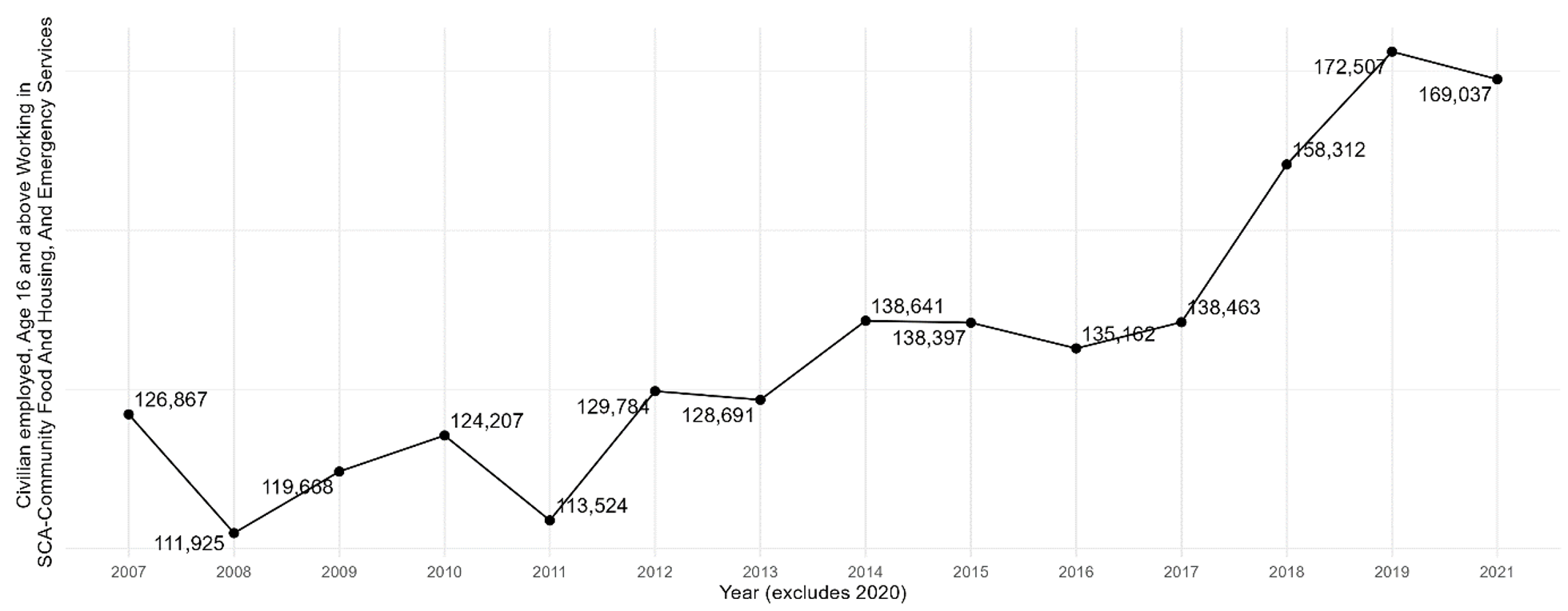
Note Includes workers aged 16 and over.
Figure B3.2 — Immigrant Share of Workers in U.S. Community Food and Housing and Emergency Services, 2007-2021
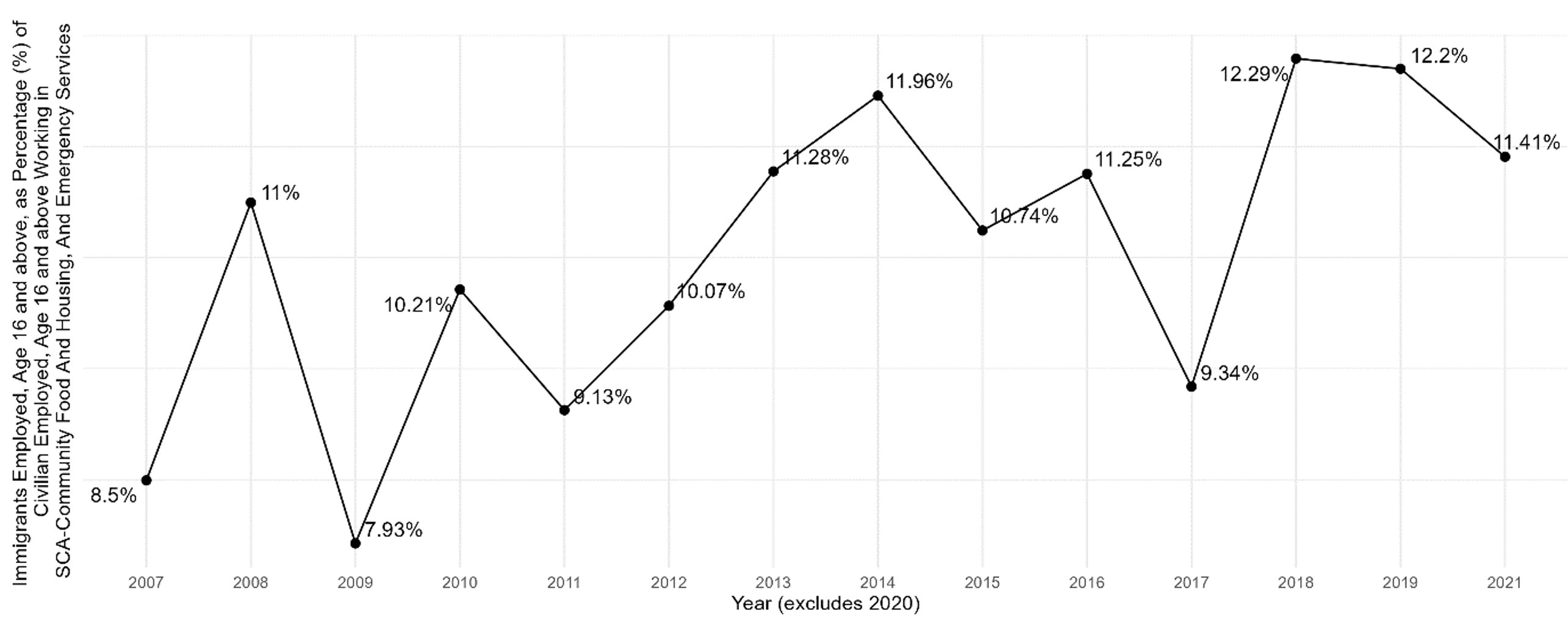
Note Includes workers aged 16 and over.
Figure B4.1 — Total Number of Workers in U.S. Vocational Rehabilitation Services, 2007-2021
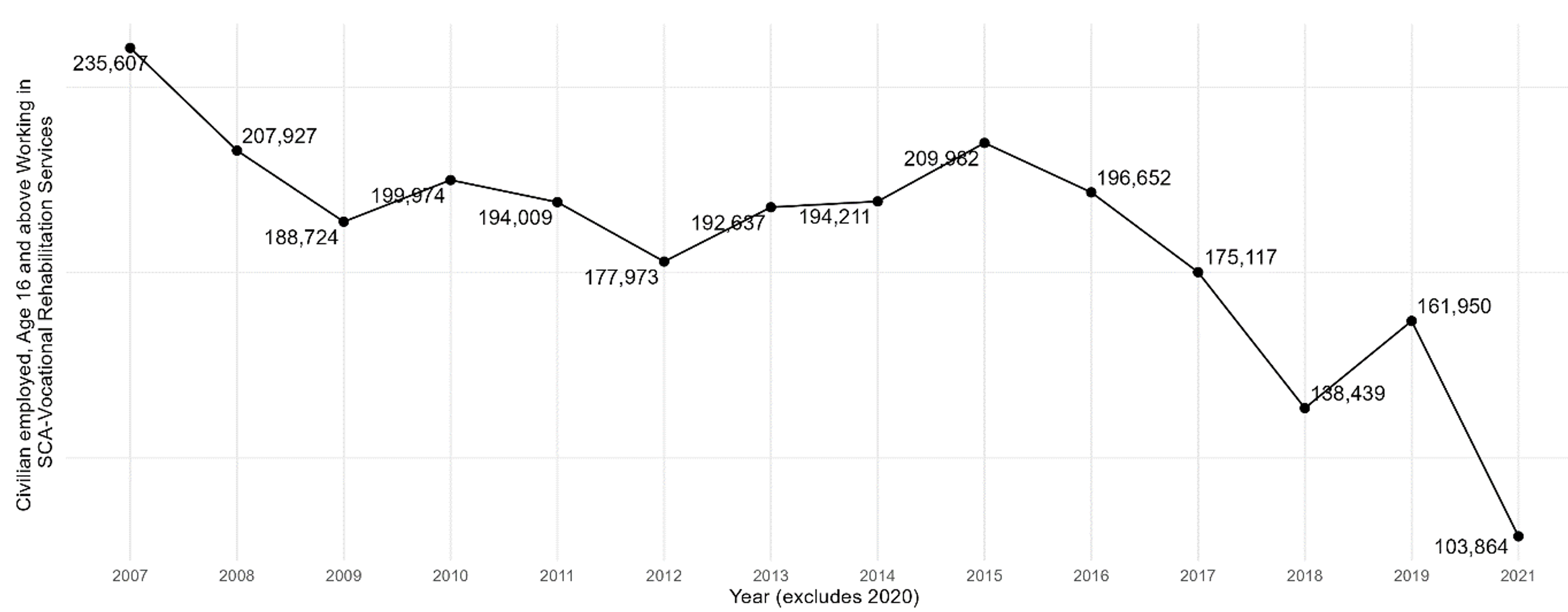
Note Includes workers aged 16 and over.
Figure B4.2 — Immigrant Share of Workers in U.S. Vocational Rehabilitation Services, 2007-2021
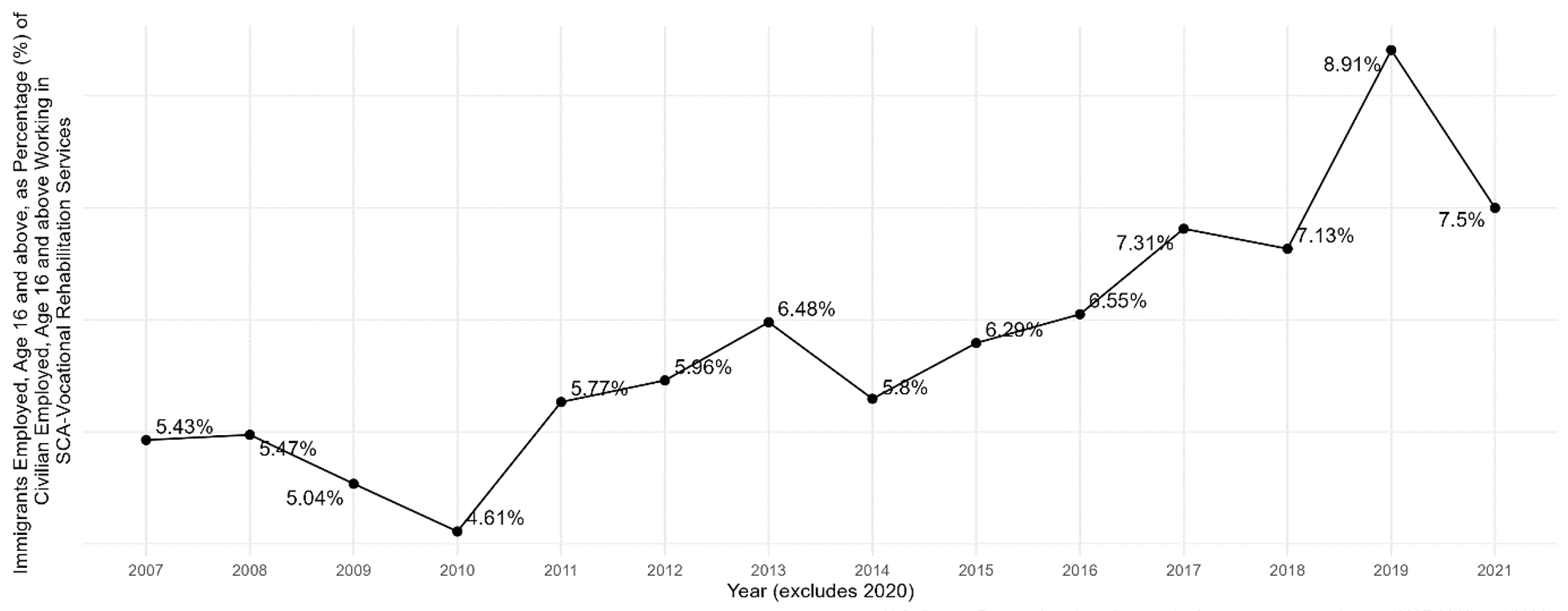
Note Includes workers aged 16 and over.
References
American Hospital Association. 2021. Strengthening the Healthcare Workforce. Washington, D.C.: American Hospital Association. https://www.aha.org/fact-sheets/2021-05-26-fact-sheet-strengthening-healthcare-workforce.
American Immigration Council. 2018. Foreign-Trained Doctors Are Critical to Serving Many U.S. Communities. Washington, D.C.: American Immigration Council. https://www.americanimmigrationcouncil.org/research/foreign-trained-doctors-are-critical-serving-many-us-communities.
Batalova, Jeanne. 2023. Immigrant Health-Care Workers in the United States. Washington, D.C.: Migration Policy Institute. https://www.migrationpolicy.org/article/immigrant-health-care-workers-united-states.
Boyle, Patrick. 2023. “Medical school enrollments grow, but residency slots haven’t kept pace.” Association of American Medical Colleges. September 3, 2020. https://www.aamc.org/news/medical-school-enrollments-grow-residency-slots-haven-t-kept-pace.
Connor, Phillip, and Abby Budiman. 2019. “Immigrant share in U.S. nears record high but remains below that of many other countries.” Pew Research Center. January 30, 2019. https://www.pewresearch.org/short-reads/2019/01/30/immigrant-share-in-u-s-nears-record-high-but-remains-below-that-of-many-other-countries/.
IHS Markit. 2021. The Complexities of Physician Supply and Demand: Projections From 2019 to 2034. Washington, D.C.: Association of American Medical Colleges. https://www.aamc.org/data-reports/workforce/data/complexities-physician-supply-and-demand-projections-2019-2034.
Martin, Brendan, Nicole Kaminski-Ozturk, Charlie O’Hara, and Richard Smiley. 2023. “Examining the impact of the COVID-19 Pandemic on Burnout and Stress Among U.S. Nurses. Journal of Nursing Regulation 14, no. 1: 4–12. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10074070/.
Martin, Susan. F. 2021. A Nation of Immigrants. Cambridge: Cambridge University Press.
Nowrasteh, Alex. and Michelangelo Landgrave. 2020. “Immigrant Health Care Workers by Occupation and State.” Cato Institute. May 13, 2020. https://www.cato.org/publications/publications/immigrant-health-care-workers-occupation-state.
Pew Research Center. 2015. Modern Immigration Wave Brings 59 Million to U.S., Driving Population Growth and Change Through 2065. Washington, D.C.: Pew Research Center. https://www.pewresearch.org/hispanic/2015/09/28/modern-immigration-wave-brings-59-million-to-u-s-driving-population-growth-and-change-through-2065/.
Singer, J. A. 2023. "Tennessee leads the way in removing barriers to foreign doctors." CATO at Liberty (blog). "https://www.cato.org/blog/tennessee-leads-way-removing-barriers-foreign-doctors.
The University of Chicago. n.d. “J-1 Status: Two-Year Home Residency Requirement & Two-Year Repeat Bar.” The Office of International Affairs. https://internationalaffairs.uchicago.edu/twoyearreq.
U.S. Bureau of Labor Statistics. 2020. “News Release: Employment Projections — 2019-2029. U.S. Department of Labor. September 1, 2020. https://www.bls.gov/news.release/archives/ecopro_09012020.pdf.
U.S. Bureau of Labor Statistics. 2020. “5 out of 20 fastest-growing industries from 2019 to 2029 are in healthcare and social assistance.” U.S. Department of Labor. September 4, 2020. https://www.bls.gov/opub/ted/2020/5-out-of-20-fastest-growing-industries-from-2019-to-2029-are-in-healthcare-and-social-assistance.htm.
U.S. Citizenship and Immigration Services. 2023. “Exchange Visitors.” Students and Exchange Visitors. https://www.uscis.gov/working-in-the-united-states/students-and-exchange-visitors/exchange-visitors.
U.S. Citizenship and Immigration Services (2020). Conrad 30 Waiver Program. https://www.uscis.gov/working-in-the-united-states/students-and-exchange-visitors/conrad-30-waiver-program.
Wolfson, J. 2023. "How Tennessee is creating new opportunities for doctors trained outside the U.S." StatNews. https://www.statnews.com/2023/05/18/doctors-trained-outside-us-licensing-tennessee/.
Young, Shannon, and Kristine White. 2023. “Hospitals ramp up foreign recruitment.” Healthcare Brew. February 22, 2023. https://www.healthcare-brew.com/stories/2023/02/22/hospitals-ramp-up-foreign-recruitment.
Endnotes
[1] U.S. Bureau of Labor Statistics, “TED: The Economics Daily,” U.S. Department of Labor, https://www.bls.gov/opub/ted/2020/5-out-of-20-fastest-growing-industries-from-2019-to-2029-are-in-healthcare-and-social-assistance.htm.
[2] For a timeline of immigration laws from 1790 to 2014, see Appendix B in Pew Research Center 2015.
[3] The health care field encompasses a broad range of professionals, including registered nurses, physicians and surgeons, health practitioner support technologists and technicians, licensed practical and licensed vocational nurses, diagnostic-related technologists and technicians, pharmacists, clinical laboratory technologists and technicians, physical therapists, emergency medical technicians and paramedics, medical records and health information technicians, speech-language pathologists, dental hygienists, dentists, miscellaneous health technologists and technicians, physician assistants, occupational therapists, respiratory therapists, dietitians and nutritionists, other health care practitioners and technical occupations, veterinarians, opticians (dispensing), chiropractors, optometrists, nurse anesthetists, recreational therapists, acupuncturists, audiologists, health-diagnosing and -treating practitioners, radiation therapists, and podiatrists. These professionals work together to provide high-quality care to patients and improve overall health outcomes.
The field of health care support includes a wide range of occupations such as nursing, psychiatric, and home health aides, medical assistants, dental assistants, massage therapists, physical therapist assistants and aides, phlebotomists, veterinary assistants and laboratory animal caretakers, medical transcriptionists, occupational therapy assistants and aides, and pharmacy aides. These professionals ensure individuals receive the care and support they need to manage their health and well-being.
[4] Physicians, also known as doctors or medical doctors, specialize in specific areas of medicine such as pediatrics, internal medicine, family medicine, psychiatry, obstetrics and gynecology, and more. They focus on nonsurgical treatments, prescribing medications, ordering diagnostic tests, and providing ongoing patient care.
Surgeons are a specialized group of physicians performing surgical procedures to treat or correct medical conditions. They are highly trained in surgical techniques and may specialize in orthopedic, cardiovascular, neuro-, plastic, or general surgery. Surgeons frequently collaborate with other medical professionals to provide comprehensive care, including preoperative assessments, surgical procedures and postoperative management.
[5] Tennessee General Assembly, H.B. 1451, https://wapp.capitol.tn.gov/apps/Billinfo/default.aspx?BillNumber=SB1451&ga=113.
This research is generously supported by a grant from the Charles Koch Foundation.
This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and Rice University’s Baker Institute for Public Policy. The views expressed herein are those of the individual author(s), and do not necessarily represent the views of Rice University’s Baker Institute for Public Policy.


